
5.4 Crisis Prevention: Help and Treatment
As the creators of the 988 Lifeline acknowledge, a crisis line is a valuable tool, but it cannot stand alone as a crisis resolution system. Rather, hotlines need to ultimately connect people to services, and more intensive levels of service need to be available and provided to people who are at high risk of engagement with the criminal justice system. Where supportive services are in place, crises involving police may be reduced, and where they fall short, crises will continue to occur and involve police contact. It is not unusual for people who end up in violent confrontations with police to later be seen as having fallen in a large “gap” between those well enough to succeed in the community with minimal support and those impaired enough to need care in a hospital (Levinson, 2021).
Earlier chapters of this text have touched on available treatment modalities and systems. Treatment in custody and via involuntary hospitalization are discussed later, in Chapter 7 and Chapter 9. What if there were more intensive and supportive forms of treatment to reach those who fall into the “gap” between more casual care and institutional care? Could this variety of treatment be part of a larger system of crisis management?
Assertive Community Treatment (ACT)
Intensive community-based treatment approaches exist, and they are proven to work. One such model, known as Assertive Community Treatment (ACT), is a model of care that has been used and studied for decades. The ACT approach allows people with serious mental disorders (such as schizophrenia) to access treatment and services in an intense model while living in their communities, thus decreasing the need for hospitalization for this population (figure 5.15). ACT is intended to be both non-restrictive and accessible. The ACT model provides a person with continuous services from a team of providers with different specialties, called a multidisciplinary team, and treatment is offered in the person’s own home (or shelter or gathering place) instead of in a clinic or office (Cunic, 2020).
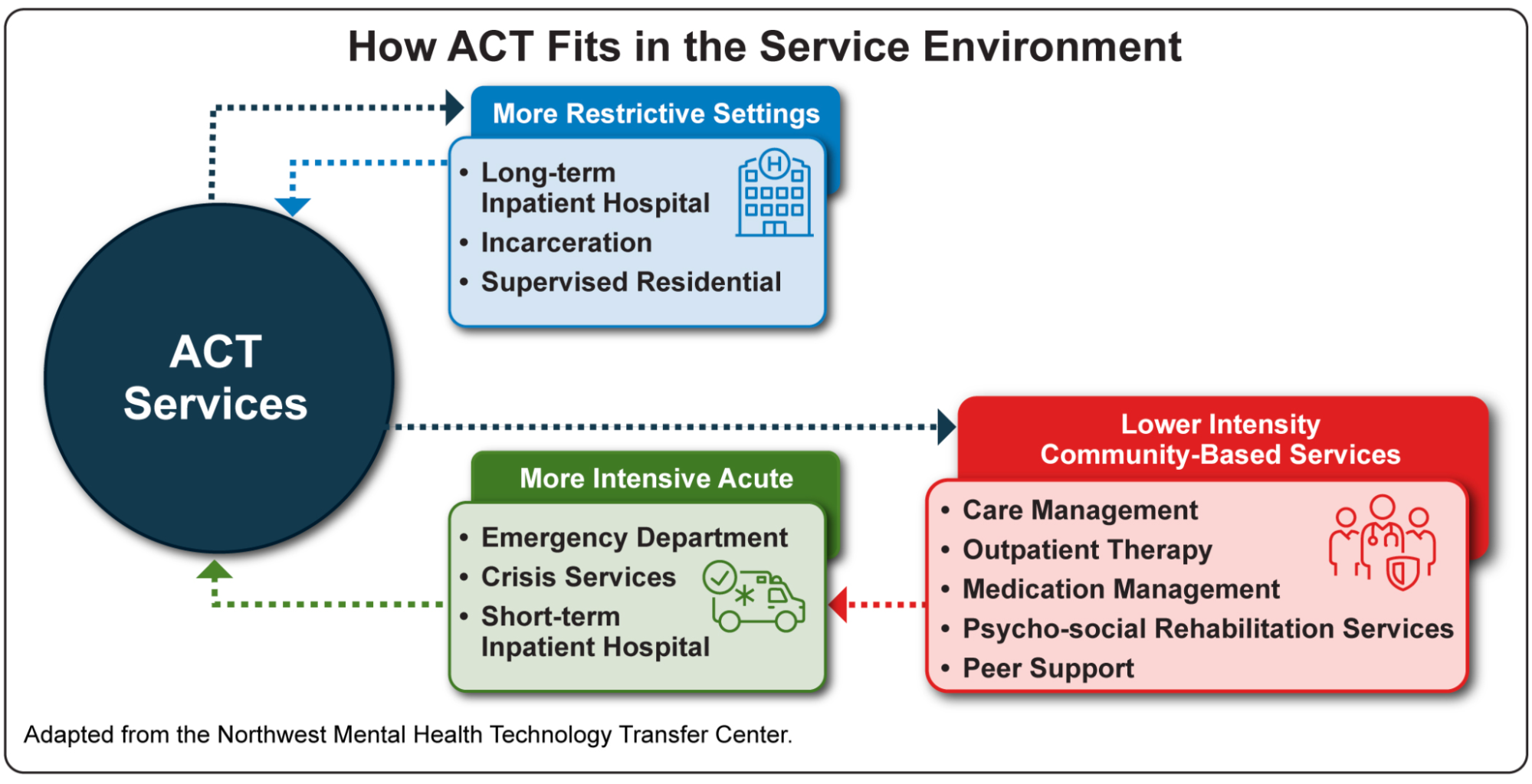
ACT treatment is intended to prevent people from having to be in a hospital and also prevent them from becoming unhoused or otherwise going into acute crisis (Cunic, 2020). The ACT team provides everything to a participating person, from assessments to psychiatric and substance abuse treatment to daily life support, including going to appointments, managing medications, and seeking or maintaining employment. ACT team members include a prescriber such as a psychiatrist or nurse practitioner, a therapist, a substance abuse specialist, a case manager, and a peer support person (The Oregon Center of Excellence for Assertive Community Treatment [OCEACT], n.d.-a). The team typically engages with a person under the ACT model around four times per week. According to the Oregon Center of Excellence for ACT, a significant number of people who engage in ACT programs eventually become ready to step down to lower levels of support (OCEACT, n.d.-b ; OCEACT, n.d.-a). If you are interested in learning more about ACT, watch the linked video produced by SAMHSA in Figure 5.16, which introduces the model.
https://www.youtube.com/watch?v=o6NtKACjwps
Forensic Assertive Community Treatment (FACT)
An extension of ACT is known as FACT, or Forensic Assertive Community Treatment. FACT (like ACT) provides community-based, continuous services via a multidisciplinary team. The forensic, or court-related, aspect of the FACT team is directed specifically toward people who have been involved in the criminal justice system—clients with serious mental illness who have been arrested/incarcerated and who have significant criminal risk. To this end, the FACT team adds criminal justice specialists, including a peer specialist with lived experience in the criminal justice system. FACT is an intervention that bridges the behavioral health and criminal justice systems (SAMHSA, n.d.).
In Multnomah County, Oregon, Cascadia Health provides FACT services. Cascadia aims FACT services at people with serious mental illness who need intensive support (e.g., a history of hospitalizations or being unhoused) and who also have repeated criminal justice involvement (e.g., frequent arrests) with “moderate to high risk to reoffend.” Cascadia’s program can serve a maximum of 45 clients drawn from a very-high needs group (Cascadia Health, n.d.-b). The qualifying level of need, in addition to capacity limits, obviously restricts the number of people who can be served in a FACT program.
While ACT and FACT are highly supportive options, these are not approaches that are available to all who might benefit. In Oregon, for example, most counties have one ACT provider, but at least six counties have none (OCEACT, n.d.-c). ACT and other intensive service models require referrals, often from hospitals or other crisis care programs.
Licenses and Attributions for Crisis Prevention: Help and Treatment
Open Content, Original
“Crisis Prevention: Help and Treatment” by Anne Nichol is licensed under CC BY-NC 4.0.
Open Content, Shared Previously
Figure 5.15. How ACT Fits In the Service Environment by SAMHSA is in the Public Domain.
All Rights Reserved Content
Figure 5.16. Assertive Community Treatment — Introductory video by SAMHSA is licensed under the Standard YouTube License.
