
12 Chapter 12 – Sexual Development Through the Lifespan
Ericka Goerling, PhD and Emerson Wolfe, MS
Learning Outcomes
- Acquire knowledge about the biological, psychological and cultural milestones in human sexual development.
- Critically differentiate between theoretical perspectives of childhood sexual development.
- Demonstrate an understanding of childhood and adolescent sexual growth and development from biological, psychological, social and cultural perspectives, and reflect on this process from a personal perspective.
- Explain how sexual values, attitudes and behavior may be expressed during the adult years within different contexts including: single living, cohabitation, marriage, consensual and non-consensual extramarital relationships, divorce, aging, widowhood.
Introduction
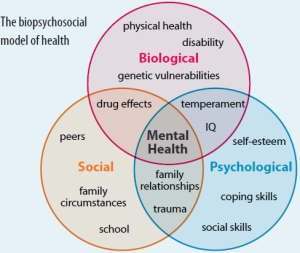
While sex and sexuality are often linked to late adolescence/early adulthood, this week’s topic explores sexuality throughout the entire lifespan. From neonatal observations to the experience of octogenarians, elements of sexuality are present throughout most of life. Although the context is surely different based on age and experience, there are still considerable domains to explore in terms of sensate experiences, genital awareness, maturation and individual and/or partnered sexual interactions. Using a biopsychosocial approach, including aspects of psychodynamic theory, we will explore elements of sex and sexuality that may occur throughout one’s lifetime. Sexual education is often taught in middle school or high school, unless an abstinence-only program is in place, but could there be benefits to openly talking about sex and being a lifelong learner when it comes to relationships and sexual satisfaction?
Theoretical Approaches
Using both a historical lens, as well as a more contemporary approach we want to first examine influential theories applied to sexuality through the lifespan. If you’ve taken any other psychology courses, you may find the following section a bit of a review since we are going to primarily discuss and apply psychoanalyst’s Sigmund Freud’s psychosexual stages of development as well as Erik Erikson’s psychosocial stages of development. As you read, consider- how do their ideas still show up in modern understanding of sexual development, including language, cultural norms, and/or values? Can you see any aspects of these theories as applied to your own experiences?
Freud’s Psychosexual Stages of Development
 Freud believed that personality develops during early childhood: Childhood experiences shape our personalities as well as our behavior as adults. He asserted that we develop via a series of stages during childhood. Each of us must pass through these childhood stages, and if we do not have the proper nurturing and parenting during a stage, we will be stuck, or fixated, in that stage, even as adults.
Freud believed that personality develops during early childhood: Childhood experiences shape our personalities as well as our behavior as adults. He asserted that we develop via a series of stages during childhood. Each of us must pass through these childhood stages, and if we do not have the proper nurturing and parenting during a stage, we will be stuck, or fixated, in that stage, even as adults.
In each psychosexual stage of development, the child’s pleasure-seeking urges, coming from the id, are focused on a different area of the body, called an erogenous zone. The stages are oral, anal, phallic, latency, and genital.
Freud’s psychosexual development theory is quite controversial. To understand the origins of the theory, it is helpful to be familiar with the political, social, and cultural influences of Freud’s day in Vienna at the turn of the 20th century. During this era, a climate of sexual repression, combined with limited understanding and education surrounding human sexuality, heavily influenced Freud’s perspective. Given that sex was a taboo topic, Freud assumed that negative emotional states (neuroses) stemmed from suppression of unconscious sexual and aggressive urges. For Freud, his own recollections and interpretations of patients’ experiences and dreams were sufficient proof that psychosexual stages were universal events in early childhood.
| Stage | Age (years) | Erogenous Zone | Major Conflict | Adult Fixation Example |
| Oral | 0–1 | Mouth | Weaning off breast or bottle | Smoking, overeating |
| Anal | 1–3 | Anus | Toilet training | Neatness, messiness |
| Phallic | 3–6 | Genitals | Oedipus/Electra complex | Vanity, overambition |
| Latency | 6–12 | None | None | None |
| Genital | 12+ | Genitals | None | None |
Oral Stage
In the oral stage (birth to 1 year), pleasure is focused on the mouth. Eating and the pleasure derived from sucking (nipples, pacifiers, and thumbs) play a large part in a baby’s first year of life. At around 1 year of age, babies are weaned from the bottle or breast, and this process can create conflict if not handled properly by caregivers. According to Freud, an adult who smokes, drinks, overeats, or bites her nails is fixated in the oral stage of her psychosexual development; she may have been weaned too early or too late, resulting in these fixation tendencies, all of which seek to ease anxiety.
Anal Stage
After passing through the oral stage, children enter what Freud termed the anal stage (1–3 years). In this stage, children experience pleasure in their bowel and bladder movements, so it makes sense that the conflict in this stage is over toilet training. Freud suggested that success at the anal stage depended on how parents handled toilet training. Parents who offer praise and rewards encourage positive results and can help children feel competent. Parents who are harsh in toilet training can cause a child to become fixated at the anal stage, leading to the development of an anal-retentive personality. The anal-retentive personality is stingy and stubborn, has a compulsive need for order and neatness, and might be considered a perfectionist. If parents are too lenient in toilet training, the child might also become fixated and display an anal-expulsive personality. The anal-expulsive personality is messy, careless, disorganized, and prone to emotional outbursts.
Phallic Stage
Freud’s third stage of psychosexual development is the phallic stage (3–6 years), corresponding to the age when children become aware of their bodies and recognize the differences between boys and girls. The erogenous zone in this stage is the genitals. Conflict arises when the child feels a desire for the opposite-sex parent, and jealousy and hatred toward the same-sex parent. For boys, this is called the Oedipus complex, involving a boy’s desire for his mother and his urge to replace his father who is seen as a rival for the mother’s attention. At the same time, the boy is afraid his father will punish him for his feelings, so he experiences castration anxiety. The Oedipus complex is successfully resolved when the boy begins to identify with his father as an indirect way to have the mother. Failure to resolve the Oedipus complex may result in fixation and development of a personality that might be described as vain and overly ambitious.
Girls experience a comparable conflict in the phallic stage—the Electra complex. The Electra complex, while often attributed to Freud, was actually proposed by Freud’s protégé, Carl Jung (Jung & Kerenyi, 1963). A girl desires the attention of her father and wishes to take her mother’s place. Jung also said that girls are angry with the mother for not providing them with a penis—hence the term penis envy. While Freud initially embraced the Electra complex as a parallel to the Oedipus complex, he later rejected it, yet it remains as a cornerstone of Freudian theory, thanks in part to academics in the field (Freud, 1931/1968; Scott, 2005).
Perhaps one of the most important take-aways from this aspect of Freud’s theory, is the unfortunate application of sexualizing children’s genital curiosity and sensate process. Children are inherently curious about their bodies at this stage of development, which is something that Freud observed. However, it’s critical to note that curiosity and even some aspects of individual or social physical exploration isn’t inherently sexual like what mature folks experience. Part of the reason this is still covered in human sexuality is to address the cultural legacy of aspects of over-sexualizing children, as well as victim-blaming (creating culpability for sexual offenses where none exists).
Latency Period
Following the phallic stage of psychosexual development is a period known as the latency period (6 years to puberty). This period is not considered a stage, because sexual feelings are dormant as children focus on other pursuits, such as school, friendships, hobbies, and sports. Children generally engage in activities with peers of the same sex, which serves to consolidate a child’s gender-role identity.
Genital Stage
The final stage is the genital stage (from puberty on). In this stage, there is a sexual reawakening as the incestuous urges resurface. The young person redirects these urges to other, more socially acceptable partners (who often resemble the other-sex parent). People in this stage have mature sexual interests, which for Freud meant a strong desire for the opposite sex. Individuals who successfully completed the previous stages, reaching the genital stage with no fixations, are said to be well-balanced, healthy adults.
While most of Freud’s ideas have not found support in modern research, we cannot discount the contributions that Freud has made to the field of psychology. It was Freud who pointed out that a large part of our mental life is influenced by the experiences of early childhood and takes place outside of our conscious awareness; his theories paved the way for others. Most importantly, the notion that early attachment matters in terms of our future personal relationships (including romantic and sexual) are domains of important modern research and application.
Erik Erikson’s Psychosocial Theory of Development
 Erik Erikson (1902–1994), another stage theorist, took Freud’s theory and modified it as psychosocial theory. Erikson’s psychosocial development theory emphasizes the social nature of our development rather than its sexual nature. While Freud believed that personality is shaped only in childhood, Erikson proposed that personality development takes place all through the lifespan. Erikson suggested that how we interact with others is what affects our sense of self, or what he called the ego identity.
Erik Erikson (1902–1994), another stage theorist, took Freud’s theory and modified it as psychosocial theory. Erikson’s psychosocial development theory emphasizes the social nature of our development rather than its sexual nature. While Freud believed that personality is shaped only in childhood, Erikson proposed that personality development takes place all through the lifespan. Erikson suggested that how we interact with others is what affects our sense of self, or what he called the ego identity.
In each stage of Erikson’s theory, there is a psychosocial task that we must master in order to feel a sense of competence.
Erikson proposed that we are motivated by a need to achieve competence in certain areas of our lives. According to psychosocial theory, we experience eight stages of development over our lifespan, from infancy through late adulthood. At each stage there is a conflict, or task, that we need to resolve. Successful completion of each developmental task results in a sense of competence and a healthy personality. Failure to master these tasks leads to feelings of inadequacy.
Although Erikson’s theory is still subject to controversies, it does have modern application to lifespan development, especially when one considers that, unlike Freud, Erikson sought to describe the entirety of a person’s life. Each of his psychosocial stages will be applied as we discuss each phase of development below. The chart below highlights Erikson’s original ideas around age and timing of developmental tasks. With advances in our understanding of brain maturation, as well as our increased lifespan, these ages may be adjusted in our discussion.
| Stage | Age (years) | Developmental Task | Description |
| 1 | 0–1 | Trust vs. mistrust | Trust (or mistrust) that basic needs, such as nourishment and affection, will be met |
| 2 | 1–3 | Autonomy vs. shame/doubt | Develop a sense of independence in many tasks |
| 3 | 3–6 | Initiative vs. guilt | Take initiative on some activities—may develop guilt when unsuccessful or boundaries overstepped |
| 4 | 7–11 | Industry vs. inferiority | Develop self-confidence in abilities when competent or sense of inferiority when not |
| 5 | 12–18 | Identity vs. confusion | Experiment with and develop identity and roles |
| 6 | 19–29 | Intimacy vs. isolation | Establish intimacy and relationships with others |
| 7 | 30–64 | Generativity vs. stagnation | Contribute to society and be part of a family |
| 8 | 65– | Integrity vs. despair | Assess and make sense of life and meaning of contributions |
Erikson’s Psychosocial Stages of Development
Sexual Development in Early Childhood
Historically, children have been thought of as innocent or incapable of sexual arousal (Aries, 1962). Yet, the physical dimension of sexual arousal is present from birth. However, to associate the elements of seduction, power, love, or lust that are part of the adult meanings of sexuality would be inappropriate. Sexuality begins in childhood as a response to physical states and sensation and cannot be interpreted as similar to that of adults in any way (Carroll, 2007).
Infancy
Boys and girls are capable of erections and vaginal lubrication even before birth (Martinson, 1981). Arousal can signal overall physical contentment and stimulation that accompanies feeding or warmth. Infants begin to explore their bodies and touch their genitals as soon as they have the sufficient motor skills. This stimulation is for comfort or to relieve tension rather than to reach orgasm (Carroll, 2007).
According to Erikson (1963), trust is the basis of our development during infancy (birth to 12 months). Therefore, the primary task of this stage is trust versus mistrust. Infants are dependent upon their caregivers, so caregivers who are responsive and sensitive to their infant’s needs help their baby to develop a sense of trust; their baby will see the world as a safe, predictable place. Unresponsive caregivers who do not meet their baby’s needs can engender feelings of anxiety, fear, and mistrust; their baby may see the world as unpredictable.
Early Childhood
Self-stimulation is common in early childhood for both boys and girls. Curiosity about the body and about others’ bodies is a natural part of early childhood. As children grow, they are more likely to show their genitals to siblings or peers, and to take off their clothes and touch each other (Okami, Olmstead, & Abramson, 1997). As toddlers (ages 1–3 years) begin to explore their world, they learn that they can control their actions and act on the environment to get results. They begin to show clear preferences for certain elements of the environment, such as food, toys, and clothing. A toddler’s main task is to resolve the issue of autonomy versus shame and doubt, by working to establish independence. This is the “me do it” stage. For example, we might observe a budding sense of autonomy in a 2-year-old child who wants to choose her clothes and dress herself. Although her outfits might not be appropriate for the situation, her input in such basic decisions has an effect on her sense of independence. If denied the opportunity to act on her environment, she may begin to doubt her abilities, which could lead to low self-esteem and feelings of shame.
Once children reach the preschool stage (ages 3–6 years), they are capable of initiating activities and asserting control over their world through social interactions and play. According to Erikson, preschool children must resolve the task of initiative versus guilt. By learning to plan and achieve goals while interacting with others, preschool children can master this task. Those who do will develop self-confidence and feel a sense of purpose. Those who are unsuccessful at this stage—with their initiative misfiring or stifled—may develop feelings of guilt.
During the preschool years, children may become increasingly aware of their bodies, which can lead to individual and peer-to-peer sexual play. Indeed physical exploration games are very common between young children, with 50 to 85 percent of kids engaging in some sort of game play that involves fantasy sexual play, exposure or stimulation of genitals (O’Donovan, 2010). How adult caregivers respond to this play can be critically important to later, mature sexual experiences.
Middle Childhood Sexual Development
Although Freud determined that middle childhood was simply a time of latency, that it’s a time when children’s sexual interests are dormant, modern understanding of sexuality tells a different story. Even Erikson noted that this stage of development is significant and that the objective is to move through industry vs. inferiority. In other words, kids are intent on gaining a sense of self and ability, of competency in their tasks and relationships. If not, Erikson argued that they may experience inferiority. With regard to sexual development, children this age may not experience the wide-eyed curiosity of their earlier years, but they also may not have entered puberty yet. Interestingly, in one survey men and women, regardless of sexual orientation, reported that the average age of their first sexual attraction was around 10 years old (Lehmiller, 2018), which reflects that there are more factors impacting school-aged children than early theory suggests.
In many western societies, school-aged children are often given their first set of educational information about their upcoming changing bodies, puberty and reproduction. For trans youth, this time can be challenging based on concerns around physical changes at the onset of puberty. Early messages about bodies, sex and sexuality can have important effects on later attitudes and behavior. There is ongoing evidence that comprehensive sex education before young people become sexually active results in a delay in the onset of sexual activity AND an increase in sexual well being (O’Donovan, 2010). Additionally, support for trans youth in terms of available health options is imperative for their ongoing physical and mental health outcomes (Turban, King, Carswell, & Keuroghlian, 2020).
Sexual Development in Adolescence
Adolescent Sexual Development
Typically, the growth spurt is followed by the development of sexual maturity. Sexual changes are divided into two categories: Primary sexual characteristics and secondary sexual characteristics. Primary sexual characteristics are changes in the reproductive organs. For males, this includes growth of the testes, penis, scrotum, and spermarche or first ejaculation of semen. This occurs around 9-14 years old (Breehl & Caban, 2020). For females, primary characteristics include growth of the uterus and menarche or the first menstrual period. The female gametes, which are stored in the ovaries, are present at birth, but are immature. Each ovary contains about 400,000 gametes, but only 500 will become mature eggs (Crooks & Baur, 2007). Beginning at puberty, one ovum ripens and is released about every 28 days during the menstrual cycle. Stress and a higher percentage of body fat can bring menstruation at younger ages. According to Breehl & Caban (2020), puberty begins on average for girls around 8-13 years old with African American girls starting puberty earlier at around 6 years old.
Stress and elevated levels of cortisol are associated with earlier puberty, especially in girls (Belsky et al., 2015). Racial microaggressions and minority stress take a toll on the body and influence mental and physical health at the intersection of race and gender (Lewis et al., 2017). In addition to most research being conducted on White girls and when they reach puberty, other health outcomes that disproportionately impact Black girls have not been researched enough (Salsbury et al., 2009). While puberty for girls of all races and ethnicities has been decreasing over the past several years, Black girls “have the lowest median age of menarche and the highest rate of childhood obesity” (Salsbury et al., 2009, p. 2). Latina youth also start puberty earlier due to similar impacts of stress and higher body mass indexes (BMIs) at a younger age (Jean et al., 2009). Something to keep in mind, research based on race and ethnic differences in pubertal timing are still very limited and it is important to question the notion of what constitutes normative BMI, especially when studies are conducted on mostly White populations. Additionally, while the timing of puberty has significant social implications which then impacts self-esteem, this interaction is also context-dependent and based on many intersecting and complex factors. Every single person may have a different experience related to puberty due to the way peers treat them and the messages they receive from the media, teachers, family, religious institutions, and more about this process.
Precocious and Delayed Puberty
If a girl begins puberty before age 8 and boys before age 9, then they would be considered to have precocious (or early) puberty (National Institute of Child Health and Human Development [NICHD], 2016). Some children may experience psychological and social problems related to feeling different than their peers (NICHD, 2016). Boys are less likely to experience negative consequences, such as bullying, if they develop earlier. Individuals who develop earlier may be perceived by others as more mature and older than they are developmentally. Thus, girls may face greater levels of sexualization earlier and boys may experience reduced levels of bullying due to their size and increased body mass.
Delayed puberty is when a girl experiences a lack of breast growth by age 13 or the lack of a period (menarche) by age 16 (Tang et al., 2020). For boys, this is when testicular enlargement has not occurred by age 14 (Tang et al., 2020). Girls and boys may experience bullying from peers due to their smaller and more child-like appearance. Boys in particular may face heightened levels of bullying and negative self-esteem consequences.
Context is Important
According to the literature review conducted by Seaton & Carter (2018), “Given ethnic/racial variations in standards of physical attractiveness, being a member of a racial group can influence body image norms. African American girls tend to describe their beauty ideals in terms of personality characteristics such as style, attitude, pride, and confidence; whereas White girls tend to describe their beauty ideals in terms of fixed physical attributes such as tall, thin, and high cheekbones… Researchers have speculated that adolescent girls who adopt body ideals in terms of personality characteristics are less vulnerable to the distress generated by puberty” (p. 42). Seaton & Carter (2018) found in their research that Black girls who view their racial identity as more central to their sense of self will experience more distress if they enter puberty later, especially if they attend a school that is predominately White. Late developing Black girls also may be further bullied by peers, so earlier puberty could act as a protection against racialized microaggressions since early maturing girls are perceived as more mature and advanced by peers within the school context (Seaton & Carter, 2018).
Jean et al. (2009) explored family dynamics and differences in acculturation between younger and older generations of Mexican Americans. The researchers found that mothers who immigrated to the United States in adulthood viewed their body size more favorably compared to their daughters who grew up attending school in the United States. Fathers were also generally very supportive of their daughters’ weight and size. Based on interviews with the girls compared to their parents, acculturation caused internalized beauty ideals that favored thinness and height more than that of their mothers and fathers. The length of time in the United States was associated with peer influence shaping standards of beauty more than family. Therefore, generational differences and acculturation can also influence body image and self-esteem. The girls who resisted acculturation actually showed more body satisfaction as their bodies began to change due to puberty when compared to the girls who internalized more American beauty standards (Jean et al., 2009).
Hormone Blockers for Transgender Individuals
An area of debate is whether transgender youth should be able to take hormone blockers prior to and during puberty in conjunction with hormone therapy in order to prevent unwanted changes during puberty and to bring about a puberty that more closely matches that of their gender identity because our society heavily correlates physical features with gender. For example, testosterone acts on the vocal cords to deepen the voice and body mass begins to redistribute which can be distressing to some transgender girls. Hormone blockers would prevent this process from occurring. However, some people argue that children cannot make such serious decisions for themselves and legally parents or guardians are the ones who consent to medical care on their youths’ behalf. This commonly results in a person needing to wait until they can consent to medical care for themselves before they can receive hormone therapy. At this point, puberty has already made lasting changes to the body that will take greater levels of medical intervention to alter.
Turban et al. (2020) and Achille et al. (2020) found that transgender youth who wanted and were provided with pubertal suppression hormones experienced a significant decrease in suicidal ideation, depression, and anxiety and reported improved overall mental health. According to Turban et al. (2020), the Endocrine Society guidelines and the World Professional Association for Transgender Health (WPATH) Standards of Care both recommend that transgender adolescents be offered puberty blockers, which are formally called gonadotropin-releasing hormone analogues (GnRHas).
People who are Intersex and Puberty
- Read “What Happens During Puberty If I’m Intersex” by Planned Parenthood (2021)
How to Support Youth Going through Puberty and Early Adolescence
- “Staying Connected: A Guide for Parents on Raising an Adolescent Daughter“- a brochure by the American Psychological Association (2001)
- “Helping Your Child through Early Adolescence” – a booklet by the US Department of Education (2005)
Adolescent Sexual Activity
By about age ten or eleven, most children experience increased sexual attraction to others that affects social life, both in school and out (McClintock & Herdt, 1996). By the end of high school, more than half of boys and girls report having experienced sexual intercourse at least once, though it is hard to be certain of the proportion because of the sensitivity and privacy of the information. (Center for Disease Control, 2004; Rosenbaum, 2006). The birth rate for teenagers has declined by 58% since 2007 and 72% since 1991, the most recent peak (Hamilton, Joyce, Martin, & Osterman, 2019). It appears that adolescents seem to be less sexually active than in previous years, and those who are sexually active seem to be using birth control (CDC, 2016).
Romantic Relationships
Adolescence is the developmental period during which romantic relationships typically first emerge. By the end of adolescence, most American teens have had at least one romantic relationship (Dolgin, 2011). However, culture does play a role as Asian Americans and Latinas are less likely to date than other ethnic groups (Connolly, Craig, Goldberg, & Pepler, 2004). Dating serves many purposes for teens, including having fun, companionship, status, socialization, sexual experimentation, intimacy, and partner selection for those in late adolescence (Dolgin, 2011). There are several stages in the dating process beginning with engaging in mixed-sex group activities in early adolescence (Dolgin, 2011). The same-sex peer groups that were common during childhood expand into mixed-sex peer groups that are more characteristic of adolescence. Straight romantic relationships often form in the context of these mixed-sex peer groups (Connolly, Furman, & Konarski, 2000). Interacting in mixed-sex groups is easier for teens as they are among a supportive group of friends, can observe others interacting, and are kept safe from a too early intimate relationship.
By middle adolescence, teens are engaging in brief, casual dating or in group dating with established couples (Dolgin, 2011). Then, in late adolescence, dating involves exclusive, intense relationships. These relationships tend to be long-lasting and continue for a year or longer, however, they may also interfere with friendships.

Although romantic relationships during adolescence are often short-lived rather than long-term committed partnerships, their importance should not be minimized. Adolescents spend a great deal of time focused on romantic relationships, and their positive and negative emotions are more tied to romantic relationships, or lack thereof, than to friendships, family relationships, or school (Furman & Shaffer, 2003).
According to the Pew Research Center (2013), individuals who identify as gay, lesbian and bisexual first realized they may not be straight around age 12, knew for sure they weren’t straight by about 17, and first told someone at about age 20. LGB+ individuals may face discrimination and bullying if they date openly depending on the specific culture and acceptance found at their school site. The prevalence of Gay-Straight Alliances and other types of supportive clubs at school sites mixed with administration and teacher support can serve as protective forces. Younger generations are also coming out much sooner compared to older generations due to society becoming more accepting overall.
Romantic relationships contribute to adolescents’ identity formation, changes in family and peer relationships, and emotional and behavioral adjustment. Furthermore, romantic relationships are centrally connected to adolescents’ emerging sexuality. Parents, policymakers, and researchers have devoted a great deal of attention to adolescents’ sexuality, in large part because of concerns related to sexual intercourse, contraception, and preventing teen pregnancies. However, sexuality involves more than this narrow focus. For example, adolescence is often when individuals who are lesbian, gay, bisexual, or transgender come to perceive themselves as such (Russell, Clarke, & Clary, 2009).
Thus, romantic relationships are a domain in which adolescents’ experiment with new behaviors and identities. However, a negative dating relationship can adversely affect an adolescent’s development. Soller (2014) explored the link between relationship inauthenticity and mental health. Relationship inauthenticity refers to an incongruence between thoughts/feelings and actions within a relationship. Desires to gain partner approval and demands in the relationship may negatively affect an adolescent’s sense of authenticity. Soller found that relationship inauthenticity was positively correlated with poor mental health, including depression, suicidal ideation and suicide attempts, especially for females.
Sexual Attraction and Sexual Identity Development
In Erikson’s terms, the time during adolescence is marked by the formation of identity versus role confusion. According to Carroll (2016), by age 14 most adolescents become interested in intimate relationships, and they may begin sexual experimentation. Many adolescents feel pressure to express interest in opposite-sex relationships, even if they are not ready to do so. This pressure can be especially stressful for those adolescents who are gay, lesbian, bisexual or questioning their sexual identity. Many adolescents who are LGB+ struggle with negative peer and family reactions during their exploration. A lack of parental acceptance especially can adversely affect the gay, lesbian or bisexual adolescent’s emerging sexual identity and can result in feelings of depression. In contrast, adolescents whose families support their sexual identity have better health outcomes.
In terms of sexual exploration with their peers, there is a fairly typical progression of behavior patterns that exists. Among Americans, the average of kissing is between 12-14, heavy petting and genital fondling occurs between 15 and 16 and average of first intercourse typically occurring between ages 16 and 18 (Lehmiller, 2018). Of course, there are numerous factors that may vary these averages (biopsychosocial factors, such as onset of puberty, physical abilities, sense of identity and/or acceptance of sexual engagement, social standing, safety, etc). Research demonstrates that the earlier teens engage in penile-vagina sex, the less likely they are to use contraception, more likely to contract a sexually transmitted infection (STI) or experience unplanned, teen pregnancy (Lehmiller, 2018). Two important notes here: First, early sexual debut doesn’t always result in negative health consequences (especially when comprehensive sex education is available). And, secondly, one of the challenges of translating sexual behaviors among all teens is that research has often limited its’ scope of inquiry to penile-vagina intercourse. Certainly, this information is relevant, yet more research into LGB+ sexual behavior, as well as cultural and societal influences in teen attitudes, are important considerations.
Sexual Development During Emerging and Early Adulthood
Emerging adulthood is the period between the late teens and early twenties; ages 18-25, although some researchers have included up to age 29 in the definition (Society for the Study of Emerging Adulthood, 2016). Jeffrey Arnett (2000) argues that emerging adulthood is neither adolescence nor is it young adulthood. Individuals in this age period have left behind the relative dependency of childhood and adolescence but have not yet taken on the responsibilities of adulthood. “Emerging adulthood is a time of life when many different directions remain possible, when little about the future is decided for certain, when the scope of independent exploration of life’s possibilities is greater for most people than it will be at any other period of the life course” (Arnett, 2000, p. 469).
Erikson’s (1950, 1968) sixth stage, intimacy versus isolation, focuses on establishing intimate relationships or risking social isolation. Intimate relationships are more difficult if one is still struggling with identity. Achieving a sense of identity is a life-long process, as there are periods of identity crisis and stability. However, once identity is established intimate relationships can be pursued. These intimate relationships include acquaintanceships and friendships, but also the more important close relationships, which are the long-term romantic relationships that we develop with another person, for instance, in a marriage (Hendrick & Hendrick, 2000).
Hooking Up
United States demographic changes have significantly affected the romantic relationships among emerging and early adults. As previously described, the age for puberty has declined, while the times for one’s first marriage and first child have been pushed to older ages. This results in a “historically unprecedented time gap where young adults are physiologically able to reproduce, but not psychologically or socially ready to settle down and begin a family and child rearing,” (Garcia, Reiber, Massey, & Merriwether, 2012, p. 172). Consequently, according to Bogle (2007, 2008) traditional forms of dating have shifted to more casual hookups that involve uncommitted sexual encounters.
Even though most research on hooking up involves heterosexual college students, 70% of sexually active 12- 21 year olds reported having had uncommitted sex during the past year (Grello, Welsh, Harper, & Dickson, 2003). Additionally, Manning, Giordano and Longmore (2006) found that 61% of sexually active seventh, ninth, and eleventh graders reported being involved in a sexual encounter outside of a dating relationship.
Hooking up Gender Differences
When asked about their motivation for hooking up, straight males and females indicated physical gratification, emotional gratification, and a desire to initiate a romantic relationship as reasons (Garcia & Reiber, 2008). In another study involving 16,288 individuals across 52 nations, males reported a greater desire of sexual partner variety than females, regardless of relationship status or sexual orientation (Schmitt et al., 2003). This difference can be attributed to gender role expectations for both males and females regarding sexual activity. Additionally, Owen and Fincham (2011) surveyed 500 college students with experience with hookups, and 65% of women and 45% of men reported that they hoped their hookup encounter would turn into a committed relationship. Further, 51% of women and 42% of men reported that they tried to discuss the possibility of starting a relationship with their hookup partner.
Thorpe and Kuperberg (2020) found that heterosexual hookups occurring within a college setting are, at least for some students, directly motivated by the unique social expectations and sexual scripts associated with attending college. In terms of motivation, women in their study were less likely than men to report hooking up as a means to improve sex skills or self-confidence (as is the case in multiple other studies). Instead, women were more likely to abstain or be motivated by possible development of romantic relationships. Interestingly, the most common motivation, which was equally cited as motivations for their last hookup by both men and women, was sexual pleasure (Thorpe & Kuperberg, 2020).
In Snapp and colleagues’ (2023) assessment of motivation among queer college student, there was a distinct aspect of pleasure that has not been as clearly outlined in the literature on heterosexual hookups. For queer college students, the motivations for hooking up have some similarities to their heterosexual peers; that is at the top of motivational factors is the want for pleasure, as well as intimacy/social relationship development, self-affirmation, and coping. Notably, however, the want for pleasure wasn’t just for self but also pleasure enhancement for their respective partners. Additionally, two other unique aspect of queer hook-ups among college students emerged; cultural norms/easy access within queer community, as well as multifaceted motives that included a mix of factors, dependent on their mood or context (Snapp, et al, 2023).
The Physiological Peak – Early Adulthood
People in their mid-twenties to mid-forties are considered to be in early adulthood. By the time we reach early adulthood, our physical maturation is complete, although our height and weight may increase slightly. Those in their early twenties are probably at the peak of their physiological development, including muscle strength, reaction time, sensory abilities, and cardiac functioning. The reproductive system, motor skills, strength, and lung capacity are all operating at their best. Most professional athletes are at the top of their game during this stage, and many women have children in the early-adulthood years (Boundless, 2016).
The aging process actually begins during early adulthood. Around the age of 30, many changes begin to occur in different parts of the body. For example, the lens of the eye starts to stiffen and thicken, resulting in changes in vision (usually affecting the ability to focus on close objects). Sensitivity to sound decreases; this happens twice as quickly for men as for women. Hair can start to thin and become gray around the age of 35, although this may happen earlier for some individuals and later for others. The skin becomes drier and wrinkles start to appear by the end of early adulthood. This includes a decline in response time and the ability to recover quickly from physical exertion. The immune system also becomes less adept at fighting off illness, and reproductive capacity starts to decline (Boundless, 2016).
Sexual Development in Middle Adulthood
Erikson’s notion of middle adulthood placed this age range between 30 and 65, though many argue that that middle aged impacts people aged 45 to 69. The psychosocial conflict, per Erikson, is generativity versus stagnation. In other words, are people experiencing a sense of continued growth and contribution or are they resigned to their lives as-is?

Sexuality is an important part of people’s lives at any age, and many middle aged and older adults are very interested in staying sexually active (Dimah & Dimah, 2004). According to the National Survey of Sexual Health and Behavior (NSSHB), (Center for Sexual Health Promotion, 2010), 74% of males and 70% of females aged 40-49 engaged in vaginal intercourse during the previous year, while 58% of males and 51% of females aged 50-59 did so.
Despite these percentages indicating that middle adults are sexually active, age-related physical changes can affect sexual functioning. For women, decreased sexual desire and pain during vaginal intercourse because of menopausal changes have been identified (Schick et al., 2010). Some may also notice less vaginal lubrication during arousal which can affect overall pleasure (Carroll, 2016; NAMS, 2024). Men may require more direct stimulation for an erection and the erection may be delayed or less firm (Carroll, 2016). Men may experience erectile dysfunction or experience a medical conditions (such as diabetes or heart disease) that impact sexual functioning.
Couples can continue to enjoy physical intimacy and may engage in more foreplay, oral sex, and other forms of sexual expression rather than focusing as much on sexual intercourse. Risk of pregnancy continues until a woman has been without menstruation for at least 12 months, however, and couples should continue to use contraception. People continue to be at risk of contracting sexually transmitted infections, such as genital herpes, chlamydia, and genital warts. In 2014, 16.7% of the country’s new HIV diagnoses (7,391 of 44,071) were among people 50 and older, according to the Centers for Disease Control and Prevention (2014e). This was an increase from 15.4% in 2005. Practicing safe sex is important at any age, but unfortunately adults over the age of 40 have the lowest rates of condom use (Center for Sexual Health Promotion, 2010). This low rate of condom use suggests the need to enhance education efforts for older individuals regarding STI risks and prevention. Hopefully, when partners understand how aging affects sexual expression, they will be less likely to misinterpret these changes as a lack of sexual interest or displeasure in the partner and more able to continue to have satisfying and safe sexual relationships.
Sexuality in the Elderly
In Erikson’s final psychosocial stage for people 70 and over, the major conflict exists with integrity versus despair. Through living life, are elderly adults able to reflect on their lives with a sense of meaning or do they feel that their regrets in life cancel out its’ importance. Indeed- this is also a time in which, based one’s physical health and well-being, where a person may still feel a genuine sense of engagement and purpose in their activities (integrity).
According to Kane (2008), older men and women are often viewed as genderless and asexual. There is a stereotype that elderly individuals no longer engage in sexual activity and when they do, they are perceived to have committed some kind of offense. These ageist myths can become internalized, and older people have a more difficult time accepting their sexuality (Gosney, 2011). For LGBT seniors, there are some significant health discrepancies, including higher rates of disability and mental distress than heterosexual older adults, as well as continued barriers to accessing healthcare (Fredriksen-Goldsen, et al, 2011). Physicians rarely inquire after elderly patients’ sexual health, lending to further challenges of sexual functioning conversations and/or STI prevention (Lehmiller, 2018).

In reality, many older couples find greater satisfaction in their sex life than they did when they were younger. They have fewer distractions, more time and privacy, no worries about getting pregnant, and greater intimacy with a lifelong partner (NIA, 2013). Results from the National Social Life Health, and Aging Project indicated that 72% of men and 45.5% of women aged 52 to 72 reported being sexually active (Karraker, DeLamater, & Schwarz, 2011). Additionally, the National Survey of Sexual Health data indicated that 20%-30% of individuals remain sexually active well into their 80s (Schick et al., 2010). For LGBTQ seniors, the Aging With Pride, The National Health, Aging, and Sexuality/Gender Study is the first federally-funded longitudinal national project designed to better understand the aging, health, and well-being of sexual and gender diverse midlife and older adults, which will yield valuable data for serving seniors.
Indeed, no matter what a person’s sexual orientation, the single biggest factor on whether someone maintains a healthy sex life in their senior years is their – and/or their partner’s – health and well-being (Lehmiller, 2018). Of important consideration is continued education on safer sex practices for seniors (Smith, et al., 2020), as well as developing strategies for managing stages of dementia and challenging sexual behavior (Fredriksen-Goldsen, et al., 2023).
Some studies indicate that sexual satisfaction declines with age, but note there are a myriad of contributing factors (Zhang, Yang, Li, & Wang, 2023). Interestingly, what seems to be the most consistent attribute to sexuality in later life, is that how sexual satisfaction gets defined shifts for people. Where early adults might find that frequency matters in terms of sexual activity, older adults determine that the quality of engagement is what matters (in other words, quality not quantity is most important).
Conclusion
Sexuality influences all of us. Throughout our lifetime, the relationship with ourselves and others may shift, sexually speaking, making the understanding of development all the more important. In this section, we’ve discussed sensate experiences from in-utero development to elderly experiences with sexuality in a way that barely covers the tip of the iceberg. Indeed – much more can be written to include the importance of social shifts in conversations around sexuality here in the US, moving from non-heteronormative research modalities (a slow work-in-progress), and how culture, race, gender and other identifications matter in our developmental processes and sexuality. Whether it’s the influence of media and technology on our sex lives or how to manage the sexual experiences of dementia patients in appropriate ways, we are still unraveling vital areas of sexual functioning. To do this adequately, we need to consistently apply biopsychosocial approaches, as well as stay curious about the many domains of sexual development.
Reflection Questions
Licenses & Attributions
Lally, M. & Valentine-French, S. (2019). Lifespan development: A psychological perspective. This textbook can be found at: http://dept.clcillinois.edu/psy/LifespanDevelopment.pdf Publication is under the following license: Creative Commons Attribution-Noncommercial-Share Alike 3.0
The content around Freud and Erikson were derived from the following OER textbook: Freud and the Psychodynamic Perspective: Psychosocial Theory of Development Created by July 31, 2018 https://www.oercommons.org/courseware/lesson/15352 Creative Commons Attribution-NonCommercial 4.0
Adaptations: Reformatted. Added learning objectives. Modified content for language, application to subject and cohesion. Updated sources.
All Rights Reserved
Desir, C. (2019). Talking to our kids about sex in the time of #metoo. TEDxOakParkWomen https://www.youtube.com/watch?v=CudqASUdCuQ&t=221s. License: All Rights Reserved. License Terms: Standard YouTube license.
Mahambrey, M. (2020). Birds and bees: Rethinking relationship and sexuality education. TEDxColumbus. https://www.youtube.com/watch?v=rE0jKANd_Po. License: All Rights Reserved. License Terms: Standard YouTube license.
Malik, R. (2022). Better sex after 65?! What predicts a great sex life in old age? https://www.youtube.com/watch?v=Y8i72EzDjmE License: All Rights Reserved. License Terms: Standard YouTube license.
Odell, S. (2022). What sex ed doesn’t tell you about the brain. TED-Ed. https://www.youtube.com/watch?v=deNGkzUlhZU. License: All Rights Reserved. License Terms: Standard YouTube license.
Sprouts Learning Co. (2017, April 23). 8 stages of development by Erik Erikson. https://www.youtube.com/watch?v=aYCBdZLCDBQ&t=72s. Licence: Published under a Creative Commons license directly on YouTube.
References
Achille, C., Taggart, T., Eaton, N. R., Osipoff, J., Tafuri, K., Lane, A., & Wilson, T. A. (2020). Longitudinal impact of gender-affirming endocrine intervention on the mental health and well-being of transgender youths: Preliminary results. International Journal of Pediatric Endocrinology, 2020(8), 1-5. This article is licensed under a Creative Commons Attribution 4.0 International License.
Belsky, J., Boyce, W. T., Ruttle, P. L., Armstrong, J. M., & Essex, M. J. (2015). Early adversity, elevated stress physiology, accelerated sexual maturation, and poor health in females. Developmental Psychology, 51(6), 816–822. https://doi-org.libproxy.pcc.edu/10.1037/dev0000017
Breehl, L., & Caban, O. (2020). Physiology, puberty. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK534827/ Publication is under the following license: Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/)
Fredriksen-Goldsen, K. I., Blueprint for Future Research Advancing the Study of Sexuality, Gender, and Equity in Later Life: Lessons Learned From Aging With Pride, The National Health, Aging, and Sexuality/Gender Study (NHAS), The Gerontologist, Volume 63, Issue 2, March 2023, Pages 373–381, https://doi.org/10.1093/geront/gnac146
Fredriksen-Goldsen, K. I., Jones, B. R., Hoy-Ellis, C., Kim, H. J., Emlet, C. A., La Fazia, D., McKenzie, G., Petros, R., & Teri, L. (2023). Aging with Pride: Innovations in Dementia Empowerment and Action (IDEA). Contemporary clinical trials communications, 35, 101169. https://doi.org/10.1016/j.conctc.2023.101169
Fredriksen-Goldsen, K. I., Kim, H.-J., Emlet, C. A., Muraco, A., Erosheva, E. A., Hoy-Ellis, C. P., Goldsen, J., Petry, H. (2011). The Aging and Health Report: Disparities and Resilience among Lesbian, Gay, Bisexual, and Transgender Older Adults – Key Findings Fact Sheet. Seattle: Institute for Multigenerational Health.
Guillory, A. (2018). Menopause. Oh Joy Sex Toy. https://www.ohjoysextoy.com/menopause/
Herbenick D, Bowling J, Fu T-C, Dodge B, Guerra-Reyes L, Sanders S (2017). Sexual diversity in the United States: Results from a nationally representative probability sample of adult women and men. PLoS ONE 12(7): e0181198. https://doi.org/10.1371/journal.pone.0181198
Jean, R. T., Bondy, M. L., Wilkinson, A. V., & Forman, M. R. (2009). Pubertal development in Mexican American girls: The family’s perspective. Qualitative Health Research, 19(9), 1210–1222. https://doi.org/10.1177/1049732309344326 Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3183834/
Lehmiller, J. J. (2018). The psychology of human sexuality (2nd ed). Wiley & Sons.
Lewis, J. A., Williams, M. G., Peppers, E. J., & Gadson, C. A. (2017). Applying intersectionality to explore the relations between gendered racism and health among Black women. Journal of Counseling Psychology, 64(5), 475–486. https://doi-org.libproxy.pcc.edu/10.1037/cou0000231
Moen, E. & Nolan, M. (2019). Sexual dysfunction. Oh Joy Sex Toys. https://www.ohjoysextoy.com/sexual-dysfunction/
National Institute of Child Health and Human Development. (2016). Puberty and precocious puberty: Condition information. https://www.nichd.nih.gov/health/topics/puberty/conditioninfo/default
O’Donovan, A. (2010). Sex and sexuality across the lifespan. In C. Butler, A. O’Donovan, & E. Shaw (Eds.), Sex, Sexuality and Therapeutic Practice: A Manual for Therapists and Trainers (p. 129–159). Routledge/Taylor & Francis Group.
Okami, P., Olmstead, R., & Abramson, P. R. (1997). Sexual experiences in early childhood: 18-year longitudinal data from UCLA Family Lifestyles Project. Journal of Sex Research, 34(4), 339-347.
Pew Research Center. (2013). A survey of LGBT Americans: Attitudes, experiences and values in changing times. https://www.pewsocialtrends.org/2013/06/13/chapter-3-the-coming-out-experience/
Salsberry, P. J., Reagan, P. B., & Pajer, K. (2009). Growth differences by age of menarche in African American and White girls. Nursing Research, 58(6), 382–390. https://doi.org/10.1097/NNR.0b013e3181b4b921 Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2876306/
Seaton, E. K., & Carter, R. (2018). Pubertal timing, racial identity, neighborhood, and school context among Black adolescent females. Cultural Diversity and Ethnic Minority Psychology, 24(1), 40-50. https://www.apa.org/pubs/journals/features/cdp-cdp0000162.pdf
Smith M. L , Bergeron C. D., Goltz H. H., Coffey T., Boolani A. (2020). Sexually Transmitted Infection Knowledge among Older Adults: Psychometrics and Test-Retest Reliability. Int J Environ Res Public Health, 17(7):2462. doi: 10.3390/ijerph17072462. PMID: 32260298; PMCID: PMC7177870.
Snapp, S. l., Ching, T. H. W., Miranda-Ramirez, M. A., Gallik, C., Duenaz, U., & Watson, R. J. (2023): Queering hookup motives in a diverse sample of LGBTQ+ young adults, The Journal of Sex Research, DOI: 10.1080/00224499.2023.2183175. https://shine.lab.uconn.edu/wp-content/uploads/sites/3321/2023/07/Snapp-et-al.-2023.pdf
Tang, C., Gondal, A. Z., & Damian, M. (2020). Delayed puberty. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK544322/ Publication is under the following license: Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/)
Thorpe, S., Kuperberg, A. (2021). Social motivations for college hookups. Sexuality & Culture 25, 623–645. https://doi.org/10.1007/s12119-020-09786-6.
Turban, J. L., King, D., Carswell, J. M., & Keuroghlian, A. S. (2020). Pubertal suppression for transgender youth and risk of suicidal ideation. Pediatrics, 145(2), e20191725. https://doi.org/10.1542/peds.2019-1725 Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7073269/
Zhang, F., Yang, Z., Li, X., & Wang, A. (2023). Factors influencing the quality of sexual life in the older adults: A scoping review. International Journal of Nursing Sciences, 10(2), 167-173.
