
15 Chapter 15 – Conception, Pregnancy, and Birth
Ericka Goerling, PhD and Emerson Wolfe, MS
Learning Outcomes
- Analyze psychosocial and cultural factors impacting abortion, pregnancy and the birthing process and discuss best practices to promote equity within healthcare systems.
- Demonstrate an understanding of the process of conception including:
- how to enhance the possibility of conception
- infertility problems and how they might be dealt with
- spontaneous and elective abortion
- aspects of a healthy pregnancy
- sexual interaction during pregnancy
- stages of childbirth
- psychological and sexual adjustments postpartum
Introduction
This week’s reading is all about conception, pregnancy and birth. Much of the content we’ll be covering will be physiological, in nature. However, as you go through the material, please keep your intersectional lens on. For example, when we’re discussing the biology of fertilization, how might environmental conditions influence the process (conception through intercourse versus IVF). Or perhaps when we consider pregnancy, how might socio-economic status and/or race impact folks’ access to prenatal care? And when we address issues of birth, note the disparity in how everything from pain care to maternal and infant mortality impact BIPOC. As with many of these topics in human sexuality, we can marvel at the complexities and wonder of our bodies and their many responses. At the same time, we can challenge the areas in which culture, race, poverty, ethnicity, abilities, and marginalization can impede some people’s opportunities.
One more note
This chapter is very much a work-in-progress. One of the challenges we’ve had authoring this chapter is finding the balance of maintaining the respectful and safe space that pregnancy and birthing has afforded generations of women. This is especially true for BIPOC communities that push back against dominant, white, medical establishments. At the same time, we seek to broaden the language, awareness, and understanding of pregnancy and birth, since so much of the traditional, western approaches have excluded gender-diverse people and families. In that vein, we are embracing the and; that is- we’re striving to consistently honor our foremothers and visionaries of birth who’ve held safe space for women, as well as respectfully embrace our non-binary, trans, and gender-diverse families in the amazing process of pregnancy and birth.
Conception
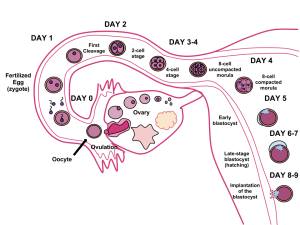
Fertilization occurs when a sperm and an oocyte (egg) combine and their nuclei fuse. Because each of these reproductive cells is a haploid cell containing half of the genetic material needed to form a human being, their combination forms a diploid cell. This new single cell, called a zygote, contains all of the genetic material needed to form a human—half from the egg and half from the sperm.
Transit of Sperm
Fertilization is a numbers game. During ejaculation, hundreds of millions of sperm (spermatozoa) are released into the vagina. Almost immediately, millions of these sperm are overcome by the acidity of the vagina, and millions more may be blocked from entering the uterus by thick cervical mucus. Of those that do enter, thousands are destroyed by phagocytic uterine leukocytes. Thus, the race into the uterine tubes, which is the most typical site for sperm to encounter the oocyte, is reduced to a few thousand contenders. Their journey—thought to be facilitated by uterine contractions—usually takes from 30 minutes to 2 hours. If the sperm do not encounter an oocyte immediately, they can survive in the uterine tubes for another 3–5 days. Thus, fertilization can still occur if intercourse takes place a few days before ovulation. In comparison, an oocyte can survive independently for only approximately 24 hours following ovulation. Intercourse more than a day after ovulation will therefore usually not result in fertilization.
During the journey, fluids in the female reproductive tract prepare the sperm for fertilization through a process called capacitation, or priming. The fluids improve the motility of the spermatozoa. They also deplete cholesterol molecules embedded in the membrane of the head of the sperm, thinning the membrane in such a way that will help facilitate the release of the lysosomal (digestive) enzymes needed for the sperm to penetrate the oocyte’s exterior once contact is made. Sperm must undergo the process of capacitation in order to have the “capacity” to fertilize an oocyte. If they reach the oocyte before capacitation is complete, they will be unable to penetrate the oocyte’s thick outer layer of cells.
Contact Between Sperm and Oocyte
Upon ovulation, the oocyte released by the ovary is swept into—and along—the uterine tube. Fertilization must occur in the distal uterine tube because an unfertilized oocyte cannot survive the 72-hour journey to the uterus.
As it is swept along the distal uterine tube, the oocyte encounters the surviving capacitated sperm, which stream toward it in response to chemical attractants released by the cells of the corona radiata. To reach the oocyte itself, the sperm must penetrate the two protective layers. Eventually, a single sperm makes contact with sperm-binding receptors on the oocyte’s plasma membrane. The plasma membrane of that sperm then fuses with the oocyte’s plasma membrane, and the head and mid-piece of the “winning” sperm enter the oocyte interior.
How do sperm penetrate the corona radiata? As you can see, the first sperm to reach the oocyte is never the one to fertilize it. Rather, hundreds of sperm cells must undergo the acrosomal reaction, each helping to degrade the corona radiata and zona pellucida until a path is created to allow one sperm to contact and fuse with the plasma membrane of the oocyte. If you consider the loss of millions of sperm between entry into the vagina and degradation of the zona pellucida, you can understand why a low sperm count can cause infertility.
The Zygote
Most of the time, a single egg is released during an ovulation cycle. However, in approximately 1 percent of ovulation cycles, two eggs are released and both are fertilized. Two zygotes form, implant, and develop, resulting in the birth of dizygotic (or fraternal) twins. Because dizygotic twins develop from two eggs fertilized by two sperm, they are no more identical than siblings born at different times.
Much less commonly, a zygote can divide into two separate offspring during early development. This results in the birth of monozygotic (or identical) twins. Although the zygote can split as early as the two-cell stage, splitting occurs most commonly during the early blastocyst stage, with roughly 70–100 cells present. These two scenarios are distinct from each other, in that the twin embryos that separated at the two-cell stage will have individual placentas, whereas twin embryos that form from separation at the blastocyst stage will share a placenta and a chorionic cavity.
In Vitro Fertilization
IVF, which stands for in vitro fertilization, is an assisted reproductive technology. In vitro, which in Latin translates to “in glass,” refers to a procedure that takes place outside of the body. There are many different indications for IVF. For example, someone may produce normal eggs, but the eggs cannot reach the uterus because the uterine tubes are blocked or otherwise compromised. There are also challenges with low sperm count, low sperm motility, sperm with an unusually high percentage of morphological abnormalities, or sperm that are incapable of penetrating the zona pellucida of an egg.
A typical IVF procedure begins with egg collection. A normal ovulation cycle produces only one oocyte, but the number can be boosted significantly (to 10–20 oocytes) by administering a short course of gonadotropins. The course begins with follicle-stimulating hormone (FSH) analogs, which support the development of multiple follicles, and ends with a luteinizing hormone (LH) analog that triggers ovulation. Right before the ova would be released from the ovary, they are harvested using ultrasound-guided oocyte retrieval. In this procedure, ultrasound allows a physician to visualize mature follicles. The ova are aspirated (sucked out) using a syringe.
In parallel, sperm are obtained from a partner or from a donor/sperm bank. The sperm are prepared by washing to remove seminal fluid because seminal fluid contains a peptide, FPP (or, fertilization promoting peptide), that—in high concentrations—prevents capacitation of the sperm. The sperm sample is also concentrated, to increase the sperm count per milliliter.
Next, the eggs and sperm are mixed in a petri dish. The ideal ratio is 75,000 sperm to one egg. If there are severe problems with the sperm—for example, the count is exceedingly low, or the sperm are completely nonmotile, or incapable of binding to or penetrating the zona pellucida—a sperm can be injected into an egg. This is called intracytoplasmic sperm injection (ICSI).

The embryos are then incubated until they either reach the eight-cell stage or the blastocyst stage. In the United States, fertilized eggs are typically cultured to the blastocyst stage because this results in a higher pregnancy rate. Finally, the embryos are transferred to the uterus using a plastic catheter (tube).
IVF is a relatively new and still evolving technology, and until recently it was necessary to transfer multiple embryos to achieve a good chance of a pregnancy. Today, however, transferred embryos are much more likely to implant successfully, so countries that regulate the IVF industry cap the number of embryos that can be transferred per cycle at two. This reduces the risk of multiple-birth pregnancies.
Pregnancy
Pregnancy begins with the fertilization of an egg and continues through to the birth of the individual. The length of time of gestation varies among animals, but is very similar among the great apes: human gestation is 266 days, while chimpanzee gestation is 237 days, a gorilla’s is 257 days, and orangutan gestation is 260 days long. The fox has a 57-day gestation. Dogs and cats have similar gestations averaging 60 days. The longest gestation for a land mammal is an African elephant at 640 days. The longest gestations among marine mammals are the beluga and sperm whales at 460 days.
Twenty-four hours before fertilization, the egg has finished meiosis and becomes a mature oocyte. When fertilized (at conception) the egg becomes known as a zygote. The zygote travels through the oviduct to the uterus. The developing embryo must implant into the wall of the uterus within seven days, or it will deteriorate and die. The outer layers of the zygote (blastocyst) grow into the endometrium by digesting the endometrial cells, and wound healing of the endometrium closes up the blastocyst into the tissue. Another layer of the blastocyst, the chorion, begins releasing a hormone called human beta chorionic gonadotropin (β-HCG) which makes its way to the corpus luteum and keeps that structure active. This ensures adequate levels of progesterone that will maintain the endometrium of the uterus for the support of the developing embryo. Pregnancy tests determine the level of β-HCG in urine or serum. If the hormone is present, the test is positive.
The gestation period is divided into three equal periods or trimesters. During the first two to four weeks of the first trimester, nutrition and waste are handled by the endometrial lining through diffusion. As the trimester progresses, the outer layer of the embryo begins to merge with the endometrium, and the placenta forms. This organ takes over the nutrient and waste requirements of the embryo and fetus, with the parent’s blood passing nutrients to the placenta and removing waste from it.
First Trimester
Internal organs and body structures begin to develop during the first trimester. By five weeks, limb buds, eyes, the heart, and liver have been basically formed. By eight weeks, the term fetus applies, and the body is essentially formed, as shown in Figure 15.4. The individual is about five centimeters (two inches) in length and many of the organs, such as the lungs and liver, are not yet functioning. Exposure to any toxins is especially dangerous during the first trimester, as all of the body’s organs and structures are going through initial development. Anything that affects that development can have a severe effect on the fetus’ survival.

Figure 15.4 Fetal development is shown at nine weeks gestation. (Credit: Ed Uthman)
Second Trimester
During the second trimester, the fetus grows to about 30 cm (12 inches), as shown in Figure 15.5. It becomes active and the mother usually feels the first movements. All organs and structures continue to develop. The placenta has taken over the functions of nutrition and waste and the production of estrogen and progesterone from the corpus luteum, which has degenerated. The placenta will continue functioning up through the delivery of the baby.
Third Trimester
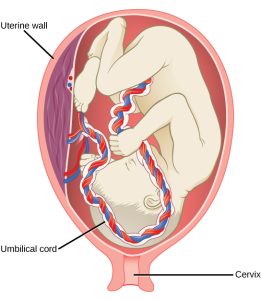
During the third trimester, the fetus grows to 3 to 4 kg (6 ½ -8 ½ lbs.) and about 50 cm (19-20 inches) long. This is the period of the most rapid growth during the pregnancy. Organ development continues to birth (and some systems, such as the nervous system and liver, continue to develop after birth).
Changes During Pregnancy
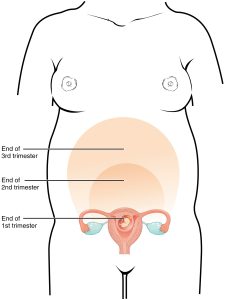
A full-term pregnancy lasts approximately 270 days (approximately 38.5 weeks) from conception to birth. Because it is easier to remember the first day of the last menstrual period (LMP) than to estimate the date of conception, obstetricians set the due date as 284 days (approximately 40.5 weeks) from the LMP. This assumes that conception occurred on day 14 of the woman’s cycle, which is usually a good approximation. The 40 weeks of an average pregnancy are usually discussed in terms of three trimesters, each approximately 13 weeks. During the second and third trimesters, the pre-pregnancy uterus—about the size of a fist—grows dramatically to contain the fetus, causing a number of anatomical changes in the pregnant person.
Weight Gain
The second and third trimesters of pregnancy are associated with dramatic changes in anatomy and physiology. The most obvious anatomical sign of pregnancy is the dramatic enlargement of the abdominal region, coupled with weight gain. This weight results from the growing fetus as well as the enlarged uterus, amniotic fluid, and placenta. Additional breast tissue and dramatically increased blood volume also contribute to weight gain (Table 15.1). Surprisingly, fat storage accounts for only approximately 2.3 kg (5 lbs) in a normal pregnancy and serves as a reserve for the increased metabolic demand of breastfeeding.
During the first trimester, the parent does not need to consume additional calories to maintain a healthy pregnancy. However, a weight gain of approximately 0.45 kg (1 lb) per month is common. During the second and third trimesters, the pregnant person’s appetite increases, but it is only necessary for them to consume an additional 300 calories per day to support the growing fetus. Contributors to Weight Gain During Pregnancy
| Component | Weight (kg) | Weight (lb) |
| Fetus | 3.2–3.6 | 7–8 |
| Placenta and fetal membranes | 0.9–1.8 | 2–4 |
| Amniotic fluid | 0.9–1.4 | 2–3 |
| Breast tissue | 0.9–1.4 | 2–3 |
| Blood | 1.4 | 4 |
| Fat | 0.9–4.1 | 3–9 |
| Uterus | 0.9–2.3 | 2–5 |
| Total | 10–16.3 | 22–36 |
Table 15.1
Changes in Organ Systems During Pregnancy
As the body adapts to pregnancy, characteristic physiologic changes occur. These changes can sometimes prompt symptoms often referred to collectively as the common discomforts of pregnancy.
Digestive and Urinary System Changes
Nausea and vomiting, sometimes triggered by an increased sensitivity to odors, are common during the first few weeks to months of pregnancy. This phenomenon is often referred to as “morning sickness,” although the nausea may persist all day. The source of pregnancy nausea is thought to be the increased circulation of pregnancy-related hormones, specifically circulating estrogen, progesterone, and hCG. Decreased intestinal peristalsis may also contribute to nausea. By about week 12 of pregnancy, nausea typically subsides.
A common gastrointestinal complaint during the later stages of pregnancy is gastric reflux, or heartburn, which results from the upward, constrictive pressure of the growing uterus on the stomach. The same decreased peristalsis that may contribute to nausea in early pregnancy is also thought to be responsible for pregnancy-related constipation as pregnancy progresses.
The downward pressure of the uterus also compresses the urinary bladder, leading to frequent urination. The problem is exacerbated by increased urine production. In addition, the maternal urinary system processes both maternal and fetal wastes, further increasing the total volume of urine.
Integumentary System Changes
The dermis (skin) stretches extensively to accommodate the growing uterus, breast tissue, and fat deposits on the thighs and hips. Torn connective tissue beneath the dermis can cause striae (stretch marks) on the abdomen, which appear as red or purple marks during pregnancy that fade to a silvery white color in the months after childbirth.
An increase in melanocyte-stimulating hormone, in conjunction with estrogens, darkens the areolae and creates a line of pigment from the umbilicus to the pubis called the linea nigra (Figure 15.8). Melanin production during pregnancy may also darken or discolor skin on the face to create a chloasma, or “mask of pregnancy.”

Figure 15.8 Linea Nigra The linea nigra, a dark medial line running from the umbilicus to the pubis, forms during pregnancy and persists for a few weeks following childbirth.
Birth
Labor is the physical efforts of expulsion of the fetus and the placenta from the uterus during birth (parturition). Toward the end of the third trimester, estrogen causes receptors on the uterine wall to develop and bind the hormone oxytocin. At this time, the baby reorients, facing forward and down with the back or crown of the head engaging the cervix (uterine opening). This causes the cervix to stretch and nerve impulses are sent to the hypothalamus, which signals for the release of oxytocin from the posterior pituitary. The oxytocin causes the smooth muscle in the uterine wall to contract. At the same time, the placenta releases prostaglandins into the uterus, increasing the contractions. A positive feedback relay occurs between the uterus, hypothalamus, and the posterior pituitary to assure an adequate supply of oxytocin. As more smooth muscle cells are recruited, the contractions increase in intensity and force.
Stages of Childbirth
The process of childbirth can be divided into three stages: cervical dilation, expulsion of the newborn, and afterbirth (Figure 15.9).
Cervical Dilation
For vaginal birth to occur, the cervix must dilate fully to 10 cm in diameter—wide enough to deliver the newborn’s head. The dilation stage is the longest stage of labor and typically takes 6–12 hours. However, it varies widely and may take minutes, hours, or days, depending in part on whether the mother has given birth before; in each subsequent labor, this stage tends to be shorter.
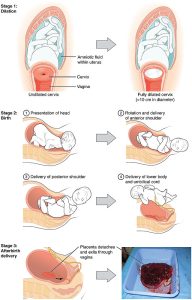
Figure 15.9 Stages of Childbirth The stages of childbirth include Stage 1, early cervical dilation; Stage 2, full dilation and expulsion of the newborn; and Stage 3, delivery of the placenta and associated fetal membranes. (The position of the newborn’s shoulder is described relative to the mother.)
True labor progresses in a positive feedback loop in which uterine contractions stretch the cervix, causing it to dilate and efface, or become thinner. Cervical stretching induces reflexive uterine contractions that dilate and efface the cervix further. In addition, cervical dilation boosts oxytocin secretion from the pituitary, which in turn triggers more powerful uterine contractions. When labor begins, uterine contractions may occur only every 3–30 minutes and last only 20–40 seconds; however, by the end of this stage, contractions may occur as frequently as every 1.5–2 minutes and last for a full minute.
Each contraction sharply reduces oxygenated blood flow to the fetus. For this reason, it is critical that a period of relaxation occur after each contraction. Fetal distress, measured as a sustained decrease or increase in the fetal heart rate, can result from severe contractions that are too powerful or lengthy for oxygenated blood to be restored to the fetus. Such a situation can be cause for an emergency birth with vacuum, forceps, or surgically by Caesarian section.
The amniotic membranes rupture before the onset of labor in about 12 percent of women; they typically rupture at the end of the dilation stage in response to excessive pressure from the fetal head entering the birth canal.
Expulsion Stage
The expulsion stage begins when the fetal head enters the birth canal and ends with birth of the newborn. It typically takes up to 2 hours, but it can last longer or be completed in minutes, depending in part on the orientation of the fetus. The vertex presentation known as the occiput anterior vertex is the most common presentation and is associated with the greatest ease of vaginal birth. The fetus faces the maternal spinal cord and the smallest part of the head (the posterior aspect called the occiput) exits the birth canal first.
In fewer than 5 percent of births, the infant is oriented in the breech presentation, or buttocks down. In a complete breech, both legs are crossed and oriented downward. In a frank breech presentation, the legs are oriented upward. Before the 1960s, it was common for breech presentations to be delivered vaginally. Today, most breech births are accomplished by Caesarian section.
Vaginal birth is associated with significant stretching of the vaginal canal, the cervix, and the perineum. Until recent decades, it was routine procedure for an obstetrician to numb the perineum and perform an episiotomy, an incision in the posterior vaginal wall and perineum. The perineum is now more commonly allowed to tear on its own during birth. Both an episiotomy and a perineal tear need to be sutured shortly after birth to ensure optimal healing. Although suturing the jagged edges of a perineal tear may be more difficult than suturing an episiotomy, tears heal more quickly, are less painful, and are associated with less damage to the muscles around the vagina and rectum.
Upon birth of the newborn’s head, an obstetrician will aspirate mucus from the mouth and nose before the newborn’s first breath. Once the head is birthed, the rest of the body usually follows quickly. The umbilical cord is then double-clamped, and a cut is made between the clamps. This completes the second stage of childbirth.
Afterbirth
The delivery of the placenta and associated membranes, commonly referred to as the afterbirth, marks the final stage of childbirth (Figure 15.10). After expulsion of the newborn, the myometrium continues to contract. This movement shears the placenta from the back of the uterine wall. It is then easily delivered through the vagina. Continued uterine contractions then reduce blood loss from the site of the placenta. Delivery of the placenta marks the beginning of the postpartum period—the period of approximately 6 weeks immediately following childbirth during which the pregnant person’s body gradually returns to a non-pregnant state. If the placenta does not birth spontaneously within approximately 30 minutes, it is considered retained, and the obstetrician may attempt manual removal. If this is not successful, surgery may be required.
It is important that the obstetrician examines the expelled placenta and fetal membranes to ensure that they are intact. If fragments of the placenta remain in the uterus, they can cause postpartum hemorrhage. Uterine contractions continue for several hours after birth to return the uterus to its pre-pregnancy size in a process called involution, which also allows the abdominal organs to return to their pre-pregnancy locations. Breastfeeding facilitates this process.
Miscarriages
Unfortunately, some instances of pregnancy do not end in a healthy birth. Miscarriage, or spontaneous pregnancy loss before 28 weeks of gestation, occurs in up to 20-25 percent of pregnancies (Sohr-Preston, Morain, Chapman, Pardue, & Ford, 2018; Bellhouse, Temple-Smith, & Bilardi, 2018). The majority of these miscarriages tend to occur before 12 weeks of gestation (often before women realize they’re pregnant). Nearly half of all miscarriages have no known cause, leading to widespread misperceptions about frequency. In cases where there is a known cause, half are attributed to chromosomal abnormalities. Consequently, most miscarriages are largely out of the control of the expectant parent. Additionally, most miscarriages do not inform the parent’s past or future success in bringing a baby to full-term (Sohr-Preston, et al, 2018).
In addition to some confusion regarding prevalence and frequency of miscarriage rates, there are often mixed responses to families impacted by miscarriage from the medical community, the general public, family members and friends. In so many ways, pregnancy loss is a time when many people need emotional support from those around them. There are a number of grass-roots agencies and hospital facilitated programs now in place to support families who’ve experienced loss. Partners are often a huge source of support, but research also identifies the need for more public discourse and education around pregnancy loss generally, which boosts well-being for all members of the families involved (Bellhouse, Temple-Smith, & Bilardi, 2018).
Abortion
The issues surrounding abortion, the deliberate termination of a pregnancy, remain highly charged throughout the United States and around the globe. In the US, there were over 600,000 abortions in 2018 reported to the Centers for Disease Control (CDC); a rate of 11.3 abortions per 1,000 women aged 15-44 years (Kortsmit, Jatlaoui, Mandel, Reeves, Oduyebo, Petersen, & Whiteman, 2020). Over half of the abortions (57.7%) in 2018 occurred among women in their 20s. Interestingly, 2018 was the first year in almost a decade where there was a slight increase in the rate of abortions (1-2% across measure). Overall, the total number of reported abortions, abortion rate, and abortion ratio decreased 22% from 2009-2018 (Kortsmit, et al, 2020). For more details on the CDC data, which outlines age of parent, gestational periods, race/ethnicity, and more can be found here and below.
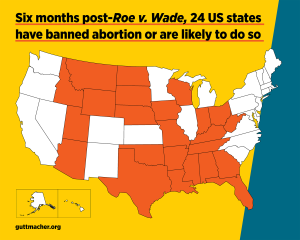
On June 24, 2022, the US Supreme Court overturned Roe v. Wade, the 1973 Supreme Court decision protecting a pregnant person’s liberty to choose to have an abortion without government prohibition. Over decades, research has demonstrated that abortion bans most severely impact people in marginalized groups who already struggle to access health care, including abortion.
Interestingly, states with the most limitations in access to abortion care also tend to have the most conservative (or absence) of sex education, the highest rates of unintended pregnancies and the lowest indicators of infant/child well-being (Dreweke, 2016; Medoff, 2018).
Caesarean Section
Cesarean section (c-sections), the surgical operation to remove an infant out of their pregnant parent’s body, has been part of human culture since ancient times (Sewel, 1998). Since 1996, c-sections have been on an almost steady rise in the United States. In 2018, approximately one-third (31.9%) of all births occurred through cesarean delivery (Martin, Hamilton, Osterman, & Driscoll, 2019). There is no question that c-sections can save lives; both of parents and children. However, there is a rising concern that many of these procedures are unnecessary, causing needless risk of complications to both mother and baby, as well as potential long-term implications (e.g. following the first c-section, there is a low probability, 10%, of later vaginal delivery; Osterman & Martin, 2014).
One of the ongoing criticisms about the high rate of c-sections is that it is primarily financially driven in terms of payout to physicians/hospitals, rather than due to patient care. Considering that a c-section costs twice as much as a vaginal delivery, the economic boon for attending medical staff/facilities can be high. On the public side of things, almost half of US births are compensated through Medicaid (with double the payout for c-sections; Kozhimannil, Graves, Ecklund, Shah, Aggarwal, & Snowden, 2018). Added to that, one meta-analysis found that c-sections are more likely to be performed on privately insured women as compared with women using public health insurance coverage (Hoxha, Syrogiannouli, Braha, Goodman, da Costa, & Jüni, 2017). Thankfully, more efforts are being examined and implemented to reduce unnecessary births via cesarean section (Kozhimannil, et al, 2018).
Disparities in Prenatal and Perinatal Care
Racial and ethnic disparities in maternal care have been an issue in the United States for generations. Just as we discussed in last week’s reading, abuse against black and brown bodies has been excessive and consequential. In terms of prenatal and perinatal care, there have been ongoing discrepancies in care, resulting in inexcusable outcomes. Nearly a quarter of black women experience delays in their prenatal healthcare and they are almost twice as likely to experience pregnancy complications (Slaughter-Acey, Sneed, Parker, Keith, Lee, & Misra, 2019).
Among industrialized nations, the US has the highest level of maternal deaths (Declercq & Zephyrin, 2020). Wang and her colleagues (2021) reported that black women are three to four times more likely to die of pregnancy-related causes compared to non-Hispanic White women. A black or indigenous person is up to 5 times more likely to die in pregnancy or up to a year after pregnancy than their white peer (Maykin & Tsai, 2020). This disparity is akin to what we saw in the 1940s (Declercq & Zephyrin, 2020).
Importantly, when controlling for other variables, such as education, socio-economic status, accessibility, findings consistently suggest that lived experiences, in the form of racial microaggressions, influence Black women’s use of health care, particularly perinatal services (Slaughter-Acey, et al, 2019). Despite advances in healthcare, antibiotics, surgical processes, and accessibility, the data provides a stark reality of rampant, systemic inequity. As Declercq and Zephyrin (2020) note, “The US has to intentionally focus on disparities between Black and white women, in particular by naming and seeking to reduce the impacts of structural racism” (p. 12). Please see the Commonwealth Fund’s recent briefing here.
There is a great deal of work to do to rectify the massive inequities facing this country. There are a variety of initiatives at both state-wide and the national level to address the disparities in perinatal care. To see a state by state comparison, go here. The Centers for Disease Control also has launched the “Hear Her Campaign.”
To be clear, the disparities in maternal health are not the result of any one, single factor. It’s at the intersection of sexism and racism, that many women of color are not being heard or seen. The initiatives noted above are a very small part in rectifying this. Continued efforts to name and eliminate structural racism, as well as provide comprehensive health care for pregnant bodies, are essential.
Conclusion
This week’s reading covers a wide range of concepts related to conception, pregnancy, and birth. Additionally, we highlighted some of the major disparities of perinatal care for BIPOC. There are other marginalized populations that need further examination; individuals with disabilities and gender nonconforming folks. There are also other stakeholders that were omitted from this section; partners, surrogates, midwives, and doulas. Finally, some considerations about lactation and postpartum adjustments can be explored further. Still, hopefully you got a solid introduction into the brilliance of conception, the marvel of pregnancy and birth, as well as the pressing issue of our time; building equity into the wrap-around healthcare of all people.
Reflection Questions
- This chapter discusses various physiological changes that occur during pregnancy. How might these changes impact a pregnant person’s daily life and experiences? Consider both physical and emotional aspects.
- Reflecting on the section about racial disparities in maternal care, what do you think are some key factors contributing to these disparities? What steps could be taken at various levels (individual, community, healthcare system, policy) to address these inequities?
- We mention the rising rates of cesarean sections in the United States. What are some potential reasons for this increase? How might the motivations behind c-sections (medical necessity vs. convenience or financial incentives) impact maternal and infant health outcomes?
- Consider the information presented about miscarriages and abortions. How do you think societal attitudes and legal frameworks surrounding these issues affect individuals’ experiences and access to care?
- This chapter briefly discusses the need for more inclusive language and considerations for diverse families, including LGBTQ+ individuals. How might the traditional focus on cisgender, heterosexual pregnancy experiences exclude or impact other groups? What changes could be made to make pregnancy and birth care more inclusive?
Licenses & Attributions
OpenStax College. (2019). Anatomy & physiology. OpenStax. http://cnx.org/content/col11496/latest/ Textbook content produced by OpenStax is licensed under a Creative Commons Attribution License 4.0 license.
OpenStax College. (2018). Biology, 2e. OpenStax. https://www.oercommons.org/courseware/lesson/15163/student/244841. Textbook content produced by OpenStax is licensed under a Creative Commons Attribution License 4.0 license.
Adaptations: Reformatted. Added learning objectives. Modified content for language, application to subject and cohesion. Updated sources. All Rights Reserved
Assefi, N. & Levine, B. A. (2015, May). How in vitro fertilization (IVF) works [Video]. https://www.ted.com/talks/nassim_assefi_and_brian_a_levine_how_in_vitro_fertilization_ivf_works?language=en. Creative Commons BY–NC–ND 4.0 International.
BabyCenter (2019, July 31). 8 positions to ease labor pain [Video]. https://www.youtube.com/watch?v=rpzBPqKgvGk&t=24s. License: All Rights Reserved. License Terms: Standard YouTube license.
Centers for Disease Control and Prevention. HearHer Campaign [Video]. https://www.youtube.com/watch?v=nxGz3naF_JQ Creative Commons Attribution 3.0 License.
Howell, E. (2019). How we can improve maternal healthcare – before, during, and after pregnancy. TEDMed. https://www.youtube.com/watch?v=XOySX6sE_8s. Creative Commons BY–NC–ND 4.0 International.
Jemyao. (2016, November 18). Miracle of life – 9 months in 4 minutes [Video]. https://www.youtube.com/watch?v=GE_lI86boUU&t=3s License: All Rights Reserved. License Terms: Standard YouTube license.
Nucleus Medical Media (2013, January 31). Fertilization [Video]. https://youtu.be/_5OvgQW6FG4 License: All Rights Reserved. License Terms: Standard YouTube license.
TEDEd (2020, October 10). The surprising effects of pregnancy [Video]. https://www.youtube.com/watch?v=F_ssj7-8rYg. Creative Commons BY–NC–ND 4.0 International.
References
Aina, A. D., Asiodu, I. V., Castillo, P., Denson, J., Drayton, C., Aka-James, R., … & Wolfe, T. (2019). Black Maternal Health Research Re-Envisioned: Best Practices for the Conduct of Research with, for, and by Black Mamas. Harv. L. & Pol’y Rev., 14, 393.
Bellhouse, C., Temple-Smith, M. J., & Bilardi, J. E. (2018). “It’s just one of those things people don’t seem to talk about…” women’s experiences of social support following miscarriage: a qualitative study. BMC women’s health, 18(1), 1-9.
Betts, J. G., Young, K. A., Wise, J. A. Johnson, E., Poe, B., Kruse, D. H., Korol, O., Johnson, J. E., Womble, M. & DeSaix, P. (2019). Anatomy and physiology. OpenStax. http://cnx.org/content/col11496/latest/
Byrnes, L., & Hickey, M. (2016). Perinatal care for women with disabilities: clinical considerations. The Journal for Nurse Practitioners, 12(8), 503-509.
Centers for Disease Control & Prevention. (2020). Hear her campaign. https://www.cdc.gov/hearher/. National Center for Chronic Disease Prevention and Health Promotion, Division of Reproductive Health.
Clark, M. A., Douglas, M. & Choi, J. (2018). Biology, 2nd Edition. OpenStax https://www.oercommons.org/courseware/lesson/15163/student/244841
Creanga, A. A., Syverson, C., Seed, K., & Callaghan, W. M. (2017). Pregnancy-related mortality in the United States, 2011–2013. Obstetrics and Gynecology, 130(2), 366. https://journals.lww.com/greenjournal/Fulltext/2017/08000/Pregnancy_Related_Mortality_in_the_United_States,.15.aspx
Declercq, E. & Zephyrin, L. (2020). Maternal mortality in the United States: A primer. The Commonwealth Fund. https://www.commonwealthfund.org/publications/issue-brief-report/2020/dec/maternal-mortality-united-states-primer
Goode, K., & Katz Rothman, B. (2017). African‐American midwifery, a history and a lament. American Journal of Economics and Sociology, 76(1), 65-94.
Guttmacher Institute. (2020). State policies on abortion. https://www.guttmacher.org/united-states/abortion/state-policies-abortion
Hoxha, I., Syrogiannouli, L., Braha, M., Goodman, D. C., da Costa, B. R., & Jüni, P. (2017). Caesarean sections and private insurance: systematic review and meta-analysis. BMJ open, 7(8).
Kortsmit, K., Jatlaoui, T. C., Mandel, M. G., Reeves, J. A., Oduyebo, T., Petersen, E., & Whiteman, M. K. (2020). Abortion surveillance—United States, 2018. MMWR Surveillance Summaries, 69(7), 1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7713711/
Kozhimannil, K. B., Graves, A. J., Ecklund, A. M., Shah, N., Aggarwal, R., & Snowden, J. M. (2018). Cesarean Delivery Rates and Costs of Childbirth in a State Medicaid Program After Implementation of a Blended Payment Policy. Medical care, 56(8), 658–664. https://doi.org/10.1097/MLR.0000000000000937
Light, A. D., Obedin-Maliver, J., Sevelius, J. M., & Kerns, J. L. (2014). Transgender men who experienced pregnancy after female-to-male gender transitioning. Obstetrics & Gynecology, 124(6), 1120-1127.
Martin, J. A., Hamilton, B. E., Osterman, M., & Driscoll, A. K. (2019). Births: Final Data for 2018. National vital statistics reports : from the Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System, 68(13), 1–47. https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_13-508.pdf
Maykin, M., & Tsai, S. P. J. (2020). Our mothers are dying: The current state of maternal mortality in Hawai ‘i and the United States. Hawai’i Journal of Health & Social Welfare, 79(10), 302.
Medoff M. (2016). Pro-choice versus pro-life: The relationship between state abortion policy and child well-being in the United States. Health Care for Women International, 37(2), 158–169. https://doi.org/10.1080/07399332.2013.841699
Obedin-Maliver, J., & Makadon, H. J. (2016). Transgender men and pregnancy. Obstetric Medicine, 9(1), 4-8.
Osterman, M. J., & Martin, J. A. (2014). Trends in low-risk cesarean delivery in the United States, 1990-2013. National vital statistics reports : from the Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System, 63(6), 1–16. https://pubmed.ncbi.nlm.nih.gov/25383560/
Sewel, J. E. (1998). Cesarean section: A brief history. https://www.nlm.nih.gov/exhibition/cesarean/index.html
Shorter, J. M., Koelper, N., Sonalkar, S., Oquendo, M. A., Sammel, M. D., & Schreiber, C. A. (2020). Racial Disparities in mental health outcomes among women with early pregnancy loss. Obstetrics and Gynecology, 137(1), 156. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7737857/
Slaughter-Acey, J. C., Sneed, D., Parker, L., Keith, V. M., Lee, N. L., & Misra, D. P. (2019). Skin tone matters: Racial microaggressions and delayed prenatal care. American Journal of Preventive Medicine, 57(3), 321-329.
Sohr-Preston, S. L., Morain, S., Chapman, A., Pardue, S., & Ford, S. (2018). Examining misperceptions about miscarriage in US adults. Journal of Prenatal & Perinatal Psychology & Health, 32(4), 285-305.
Wang, E., Glazer, K. B., Sofaer, S., Balbierz, A., & Howell, E. A. (2020). Racial and ethnic disparities in severe maternal morbidity: A qualitative study of women’s experiences of peripartum care. Women’s Health Issues. https://www.sciencedirect.com/science/article/pii/S1049386720301006?casa_token=_cuyMu_v-BQAAAAA:0wixvLium4n7tUwzlW6oYwqcAIXxzX-xbJjgODfzFMTxXIP_39BrKuvOYKhM06_NUIEuQ_crlg
