
4 Histology of tooth and periodontal tissues
- Overview
- Bone tissue review
- Histology of teeth
- Enamel
- Dentin
- Pulp
- Histology of periodontal tissues
- Cementum
- Periodontal Ligament
- Alveolar bone
- Summary of hard tissues
Overview
This chapter briefly covers the histology of the hard tissues enamel, dentin, cementum and bone, as well as the soft tissues of pulp and the PDL. The definitions and clinical considerations of these tissues are covered in chapters on the development of these tissues (Chapters 8 through 11)
For more practice using histology images, we share these useful links
- The
Oral histology lab- by Brian R. MacPherson, Ph.D. and James G. Tieman, Ed.D., at the University of Kentucky (we linked to this in the previous chapter as well)
- The
Microanatomy Web Atlas- by Gwen V. Childs, Ph.D., FAAA at the
University of Arkansas for medical sciences. Jump to the digestive system/tooth unit.
- by Gwen V. Childs, Ph.D., FAAA at the
Histology of bone tissue (short review)
Bone tissue← is deposited in layers by osteoblasts. These cells become trapped inside lacunae between layers of bone tissue, and differentiate← into osteocytes. Bone tissue can either be compact and made of osteons, or spongy bone made of trabeculae. Bone tissue is almost entirely ECM, summarized in Table 4.1. Bone tissue is highly vascular—compact bone contains central canals and perforating canals, whereas in spongy bone the space between bony trabeculae is filled with red bone marrow or highly vascular adipose connective tissue.
| Components of bone tissue | |
|---|---|
| <1% | Osteocytes |
| 66% | Mineral ECM: Calcium Hydroxyapatite |
| 33% | Protein ECM: Collagen |
Histology of teeth
Histology of enamel
Enamel shares some mineral characteristics with bone tissue, but it is acellular and avascular. Enamel matrix is deposited in columns called enamel rods by cells called ameloblasts. Enamel is the strongest substance in the human body, due to its high mineral content, listed in Table 4.2. Like bone tissue, the ECM is mostly calcium hydroxyapatite, but instead of collagen← fibers, enamel contains proteins including amelogenins and enamelins.
| Components of enamel | |
|---|---|
| 0.0% | Cells (there are no cells) |
| 96% | Mineral ECM: Calcium Hydroxyapatite |
| 4% | Protein ECM: Amelogenins and Enamelin (not collagen)
Water |
Tooth of Paranthropus robustus SKX 21841 from Swartkrans" by Didier Descouens, is licensed CC BY 3.0 / boxes and animation addedDuring embryonic development, ameloblasts work on a circadian rhythm, depositing ECM at a regular pace for 4 days, then changing speed. The changes in speed lead to changes in enamel density, which can be seen as horizontal Lines of Retzius (or Striae of Retzius). Another pattern is visible because ameloblasts do not create an enamel rod in a perfectly straight line, but change direction slightly over days. This leads to the pattern known as Hunter-Schreger bands. The border between enamel and underlying dentin is a distinct line named the dentin-enamel junction (DEJ). Ameloblasts are lost during tooth eruption←, and are therefore not found in the adult tissue. As a result, enamel does not undergo remodeling the way the remodeling unit maintains bone tissue throughout life.
"Dentinal tubule occlusion of dentine discs after treatment" by Peiyan Yuan, is licensed CC BY SA 3.0 / labels, arrows and animation addedHistology of dentin
Dentin, like enamel, is avascular, but it should not be called acellular. Dentin matrix is deposited by cells called odontoblasts. These cells—or more accurately, their cell bodies– are found within the pulp cavity, immediately adjacent to the dentin. Each odontoblast has an arm-like protrusion called an odontoblastic process that extends nearly the entire thickness of the ECM that cell secreted. The odontoblastic process secretes more dentin (in a soft form that hardens later), as well as a fluid called dentinal fluid into the space known as a dentinal tubule. Dentin is not as strong as enamel, because of its lower mineral content, listed in Table 4.3. Dentin makes up the greatest bulk of teeth.
| Components of dentin | |
|---|---|
| – | Cells (odontoblasts cell bodies in pulp, odontoblastic processes in dentin) |
| 70% | Mineral ECM: Calcium Hydroxyapatite |
| 30% | Protein ECM: Collagen, mostly
Water |
"histological section of tooth" by Doc. RNDr. Josef Reischig, CSc. is licensed under CC BY-SA 3.0 / labels and animations addedSimilar to the Lines of Retzius, dentin is deposited at different rates over days, which creates bands called the Imbrication lines of von Ebner. These lines run perpendicular to the dentinal tubules. Exceptionally-pronounced imbrication lines are named the Contour lines of Owen, and occur with changes in nutrition (such as during childbirth).

Root dentin has a layer of speckles near the border with the cementum named Tomes' granular layer. It has no known function. It is a good landmark when looking at dentin under the microscope, its presence indicates you are viewing root dentin, not mantle dentin, and a thin layer of cementum should be close by.
Histology of pulp
The pulp chamber is composed of an indeterminate type of connective tissue, although it most resembles areolar connective tissue←. The most common cell types found within the pulp core are fibroblasts and mesenchymal stem cells. The pulp houses the blood, nerve and lymphatic supplies for each tooth. The pulp has 4 layers that appear distinct when using an H&E stain, listed in Table 4.4.
| Layer | Predominant feature |
|---|---|
| Odontoblast layer | Odontoblast cell bodies |
| Cell-free zone | Not actually free of cells, cells aren’t visible |
| Cell-rich zone | Cells are visible and densely packed |
| Pulp core | Location of capillaries, nerve endings and lymphatic vessels |
Histology of periodontal tissues
Histology of cementum
Cementum forms a thin layer (between 50 to 200 μM, see below) over the surface of root dentin, which is roughly the width of a hair. The ECM of cementum differs significantly enough from enamel that the two can be differentiated by their color (cementum is yellowish in hue, enamel has no color). Both cementum and dentin are yellowish, making those two difficult to differentiate by color. The ECM of cementum is deposited by cementoblasts, which can be found on the surface of cementum throughout life. As a result, the thickness of cementum can triple in thickness between the ages of 10 and 70 years of age. This is not the same as bone remodeling, as it does not involve the activity of resorptive cells in addition to cementoblasts. Cementum incorporates more fluoride than the other hard tissues.
Cementum, like dentin and enamel, is an avascular tissue, but it can contain cells. There are two types of cementum based on histological (visual) studies from the 1830s: cellular cementum and acellular cementum. More recent advances in molecular biology and genetics are yielding newer concepts, but the old classification system is still commonly used in clinical practice.
In cellular cementum, cementoblasts become trapped within the ECM and differentiate← into cementocytes. In the mature tissue, cementocytes are found within lacunae, similar to bone tissue←. However, canaliculi only extend in the direction of the (vascular) PDL. In the opposite direction is avascular dentin, which cannot provide cementocytes with nutrients. Cellular cementum is found in the apical half of the root.
Acellular cementum does not contain cementocytes, and can be found in the coronal half of the root as well as underneath cellular cementum in the apical portion (cementum is around 50 μM thick in the coronal region and 200 μM thick in the apical region).
The border between cementum and dentin, the Cementum-Dentin junction (CDJ), is less distinct than the DEJ. Cementum is slightly less strong than dentin, and is composed of the materials listed in Table 4.5. Some publications list the mineral component of cementum to be 60 to 65% (further reading here). The difference between these numbers reflects whether a layer of mostly un-mineralized glycoproteins at the CDJ is included or excluded. The glycoproteins are specific to cementum, therefore we have chosen to report measurements that include them.
Regardless of how we measure the mineral content of cementum, loss of bone, dentin and cementum in response to periodontitis and orthodontia← is complex and requires discussion of morphogens← and the differentiation← of resorptive cells. Similarly, discussion of whether cementum should be categorized as a part of the tooth (based on its location and appearance) or a part of the periodontium is best left until we discuss the lineage of tooth and periodontal tissues.
| Components of cementum | |
|---|---|
| – | Cellular cementum (apical portion)
Acellular cementum (coronal portion) |
| 50% | Mineral: Calcium Hydroxyapatite |
| 50% | Protein: Collagen and glycoprotein mixture
Water |
Fibers in cementum

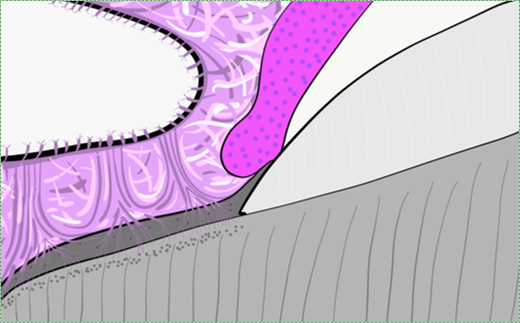
"Schematic diagram depicting how cementoblasts produce intrinsic fibers around principal fibers on extrinsic fiber-rich CIFC." by Tsuneyuki Yamamoto et al, Jpn Dent Sci Rev is licensed under CC BY-NC-ND 4.0Acellular cementum contains extrinsic collagen fibers which travel perpendicular to the surface of the root, and are likely secreted by both fibroblasts and cementoblasts. These fibers connect all the way to alveolar bone, and represent the ends of the principal fibers of the PDL embedded within cementum (extrinsic fibers may be called Sharpey’s fibers, the same as bone tissue).
Cellular cementum contains intrinsic fibers and possibly extrinsic fibers. Intrinsic collagen fibers are secreted by cementoblasts, and do not extend beyond cementum. They are oriented parallel to the root surface and are mainly involved in the repair of cementum (a scaffold←). More recent publications subdivide cellular cementum into Cellular Intrinsic Fiber Cementum and Cellular Mixed Stratified Cementum, based on the amount of extrinsic collagen fibers present. Cementum that does not contain extrinsic collagen fibers (closer to the cervical region) does not contribute to the attachment to bone tissue.
Histology of the Periodontal Ligament
The Periodontal Ligament (PDL) is a region of dense regular connective tissue← that connects the cementum to alveolar bone. Sharpey's fibers extend from one side of the PDL into cementum, and on the other side of the PDL into alveolar bone. Like the CDJ, the border between cementum and PDL is blurred due to their shared lineage. Clusters of rogue epithelial cells can be found within the PDL which are named the epithelial rests of Malassez. The PDL has a much higher degree of vascularity than other ligaments. It also has a more diverse and numerous population of cells (compare Fig. 4.14 to the link to dense regular connective tissue above).
Histology of alveolar bone
Alveolar bone contains compact bone tissue, with a semi-unique feature of many tiny holes through which Sharpey's fibers from the PDL insert, as well as larger holes for the nerves, blood and lymphatic vessels that exit bone tissue and enter the apical foramen of a tooth. This makes the surface of the alveolar sockets appear porous, which is almost unique for the surface of bones. The porous surface is called the cribriform plate, which is not to be confused with the other region of compact bone riddled with tiny holes, the cribriform plate of the ethmoid bone (whose holes are for olfactory nerve endings, connecting the nasal cavity to the brain).
Resorptive cells in hard tissues
The periosteum is a layer of dense regular connective tissue← that surrounds bone tissue. In addition to collagen← fibers, it contains osteoblasts and osteoclasts involved in bone remodeling←. Similar cells exist for cementum and dentin, but not enamel. Cementoclasts and odontoclasts are capable of demineralizing cementum and dentin, respectively. Like osteoclasts, these cells express genes involved in acid secretion as well as digestive enzymes, including members of the matrix metalloproteinase family. Unlike osteoclasts, they are not active continuously in a remodeling unit, they have no baseline activity and are typically only activated during tooth exfoliation.
Odontoclasts and cementoclasts likely differentiate← from the same bone marrow stem cells← that become osteoclasts. The signals that determine whether the multi-potent stem cell differentiates into an osteoclast, odontoclast or cementoclast are currently not well understood. The body may regulate this process by long or medium-range hormone and growth factor signals. Regulation may also be very short-range: binding of the stem cell to proteins or glycoproteins within the ECM of each target tissue, providing the stem cell with positional information. While roughly identical to osteoclasts under the microscope, odontoclasts and cementoclasts have important physiological differences. For instance, the hormone calcitonin inhibits osteoclasts but triggers odontoclast activity during root resorption. The significance of this detail is that root resorption does not always match bone resorption. For instance, in osteoporosis, it is bone resorption, not tooth root resorption, that leads to the loss of teeth. During tooth exfoliation, however, root dentin is resorbed but alveolar bone undergoes both resorption and deposition, to form a pathway through bone above the permanent tooth and fill in alveolar socket space below.
Some publications suggest cementoclasts are distinct cells found in the PDL and that they play a role in the maintenance of cementum throughout life. Other publications suggest cementoclasts are the same cell type as odontoclasts and osteoclasts. Without further study, it is hard to tell whether a cementoclast is a distinct cell type, or an osteoclast found near cementum. The difference may be semantic, like asking whether your teacher is still a teacher when you see them in the grocery store, or are they just another shopper? The mechanism of resorption is the same (acids and proteinases), but whether these cell are regulated the same is an important question during tooth exfoliation and orthodontic movement←.
Summary of hard tissues
>
| Hard tissue | Components | |
|---|---|---|
| Enamel | 96% | Mineral: Calcium Hydroxyapatite |
| 1% | Protein: Amelogenins and Enamelins (not collagen) | |
| 3% | water | |
| Dentin | 70% | Mineral: Calcium Hydroxyapatite |
| 20% | Protein: Collagen, mostly | |
| 10% | water | |
| Cementum | 50%* | Mineral: Calcium Hydroxyapatite |
| 50%* | Protein: Collagen and glycoprotein mixture
Water |
|
| Bone | 60% | Mineral: Calcium Hydroxyapatite |
| 25% | Protein: Collagen | |
| 15% | water | |
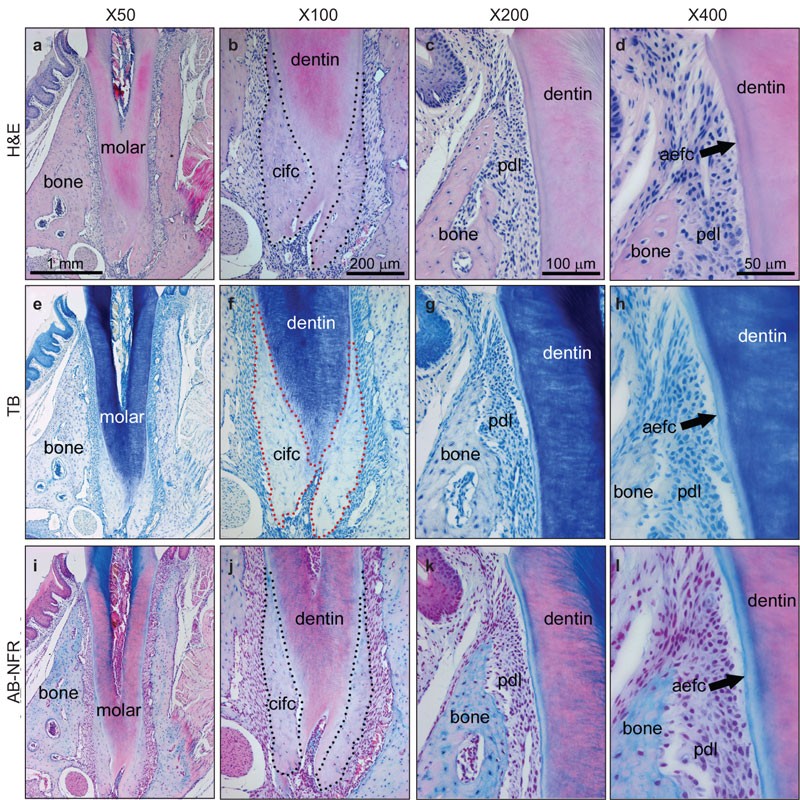
"Serial sections of the 44 dpn mouse mandibular first molar were stained with (a–d) H&E, (e–h) TB and (i–l) AB-NFR" by Brian L Foster is licensed under CC BY-NC-ND 4.0< Chapter 3 *navigation * Chapter 5 >
Chapter review questions
Periodontal Ligament, a group of specialized connective tissue fibers that attach a tooth to alveolar bone.
A hard connective tissue which is mostly ECM, including collagen fibers and a calcium-phosphate crystal.
A differentiated connective tissue cell that secretes bone ECM, including collagen, calcium and phosphate.
Lakes, or spaces within cartilage of bone connective tissue where cells reside.
When one cell begins to look different from another. This process involves limiting cell fate by altering gene transcription to become more specialized.
The terminally differentiated cell type found in mature bone tissue (both compact and spongy), capable of repairing small amounts of damage.
Rod-like mineralized connective tissue structures found in spongy-bone.
Extra-Cellular Matrix: Materials in the body, but outside of cells. A network of macromolecules, such as fibers, enzymes, and glycoproteins, that provide structural and biochemical support to surrounding cells.
Containing blood vessels
A type of connective tissue composed primarily of adipocytes, which store high-energy triglyceride and other lipid molecules.
Without cells
Without blood vessels
The basic unit of tooth enamel, 4 μm wide, composed of a tightly packed and organized mass of hydroxyapatite crystals, hexagonal in shape.
Cells present only during the embryonic period that deposit tooth enamel.
Ca5(PO4)3(OH), the inorganic ECM material composed of calcium, phosphate and hydroxide ions that makes up the bulk of bone tissue.
The main structural protein in the ECM of connective tissues
Proteins found in enamel matrix which regulate the initiation and growth of hydroxyapatite crystals during the mineralization of enamel.
Along with amelogenins, a second protein found in enamel, enamelins are necessary for the adhesion of ameloblasts to the surface of the enamel, and they bind to hydroxyapatite to promotes crystallite elongation.
Incremental growth lines seen in enamel.
When cut enamel is viewed under reflected light, curves in the pattern of enamel rods can be seen; these curves strengthen the enamel and prevent cracks from propagating through the tooth.
Dentin-Enamel Junction
A process in tooth development in which the teeth enter the mouth and become visible.
Reorganization or renovation of existing tissues, either physiological or pathological. The process can either change the characteristics of a tissue such as in blood vessel remodeling, or result in the dynamic equilibrium of a tissue such as in bone remodeling.
Osteoblasts and osteoclasts working together to remove old bone tissue and replace it with new bone tissue, necessary for the maintenance of healthy bones.
A cell of neural crest origin that is part of the outer surface of the dental pulp, and whose biological function is the formation of dentin.
Arm-like extension of an odontoblast found within dentinal tubules.
The lymph or ECF found within dentinal tubules, surrounding the odontoblastic process
Tiny canals that run through dentin, from the pulp cavity up to near the DEJ or CDJ
Incremental lines in the peritubular dentin of the tooth that correspond to the daily rate of dentin formation.
Exceptionally-pronounced imbrication lines of von Ebner
A layer of dark granules that lie parallel to the outer surface of root dentin.
The outer layer of dentin closest to enamel, contains few odontoblastic processes.
A loose connective tissue composed of fibroblasts and other cell type, plus ground substance and all three fiber types.
The basic connective tissue cell type capable of secreting ECM components, including fibers and ground substance proteins.
Multipotent cells of a connective tissue that can differentiate into a variety of cell types, including osteoblasts, fibroblasts, chondrocytes, myoblasts, blood cells and adipocytes.
Hematoxylin and Eosin stain, typically turns proteins pink and DNA purple.
Differentiated cell that deposits cementum matrix.
Cells capable of removing a tissue, such as osteoclasts, cementoclasts and odontoclasts.
Cementum containing cells and collagen fibers anchoring the tooth to alveolar bone.
Cementum covering the cervical portion of the tooth root, important for attachment of the periodontal ligament (PDL) to the root surface.
Terminally differentiated cell found within mature cementum lacunae.
Microscopic canals between the lacunae of ossified bone or cementum, containing thin cell processes linking distant cells together.
Cementum-Dentin Junction
A protein that has had sugar residues attached to it in the Golgi apparatus and is often secreted.
Inflammation that damages soft tissue and bone that anchors the teeh, including the gingiva plus PDL, cementum or alveolar bone tissue.
The treatment of irregularities in the teeth (especially of alignment and occlusion) and jaws, including the use of braces.
A substance whose non-uniform distribution governs the pattern of tissue development and pattern formation.
Specialized tissues that surround and support the teeth, including gingival tissue, PDL, cementum and alveolar bone.
The developmental history of a differentiated cell traced back to the embryonic cell from which it arises.
Ends of the principal fibers of the periodontal ligament embedded within cementum.
The main principal fiber group is the alveolodental ligament, which consists of five fiber subgroups: alveolar crest, horizontal, oblique, apical, and interradicular on multirooted teeth. Principal fibers other than the alveolodental ligament are the transseptal fibers.
Bundles of strong type I collagen that anchor the periosteum to bones by penetrating the outer layers of compact bone tissue
Fibers found within cementum oriented parallel to the root surface, mainly involved in the repair of cementum.
Extracellular matrix material involved in the repair of injured and missing tissues, allows stem cells to migrate into the injured area. It is usually replaced during regeneration.
A type of connective tissue found in tendons and ligaments that is composed primarily of parallel collagen fibers, secreted by fibroblasts, with very little ground substance.
The part of the jaws that holds the teeth.
Clusters of epithelial cells found within the PDL, remnants of Hertwig's Epithelial Root Sheath (HERS).
Sieve-like region of compact bone of the alveolar sockets or ethmoid bone.
A layer f dense regular connective tissue surrounding bones, also containing osteoblasts, osteo-progenitor cells and some osteoclasts.
A cell derived from bone marrow stem cells capable of demineralizing bone tissue by the secretion of acids and enzymes, releasing calcium into the blood.
Resorptive cell capable of demineralizing cementum by the secretion of acids and enzymes.
Resorptive cell capable of demineralizing dentin by the secretion of acids and enzymes.
Enzymes that degrade all kinds of extracellular matrix proteins, or process a number of bioactive molecules. They play a major role in cell proliferation, migration, differentiation, angiogenesis, and apoptosis.
A general term for peeling or shedding, in humans it refers to the loss of dead epithelial cells or structures (hair, teeth).
Undifferentiated or partially differentiated cells that can differentiate into various cell types, and proliferate to produce more of the same stem cell.
Signaling molecules secreted directly into the blood which travel throughout the body.
A signaling molecule capable of stimulating cell proliferation, wound healing, and cellular differentiation.
In pattern formation, the development of spatial organization in the embryo that results from cells differentiating at specific positions, which requires that the cells have positional values as in a coordinate system

{kind=link}
_Histologic_section_of_tooth.jpg){kind=link}