
Inhaled Medications & Nebulizers
Inhaling substances is a fast-acting way to get a drug into the body. The speed and ease of administration make this route a preferred method of illicit drug use as well as a great way to administer lifesaving breathing treatments. There are three main ways the EMT administers inhaled medications: Metered-Dose Inhaler, Medication Nebulizer, and Medication Mask Nebulizer.
Metered-Dose Inhaler (MDI) – These are widely available to the public through prescriptions for Asthma and COPD. The primary medication administered through an MDI is Albuterol (see Albuterol). There are other inhaled medications available, but Albuterol is the only MDI medication EMTs can assist in administering.
To assist a patient with administering MDI device:
- Ensure the patient is suffering from a condition warranting administration (Asthma, COPD, etc.).
- Ensure its the correct medication & that it is prescribed to that patient.
- Identify the availability of a spacer.
- Shake MDI for approx. 10 seconds.
- Instruct patient to exhale completely.
- Place inhaler mouth port in patient’s mouth.
- Instruct patient to breathe in fully.
- As the patient breathes in, press the inhaler down to release medication.
- Instruct patient to hold breath as long as possible.
- Repeat as necessary up to limit by protocol & scope of practice.

Medication Nebulizer “Med-Neb” – These are generally only available to patients with severe asthma or COPD. They may be carried on your ambulance or rescue unit and are readily available with ALS services. Some assembly is required, and this device requires oxygen to deliver medications.
To set up a Med-Neb:
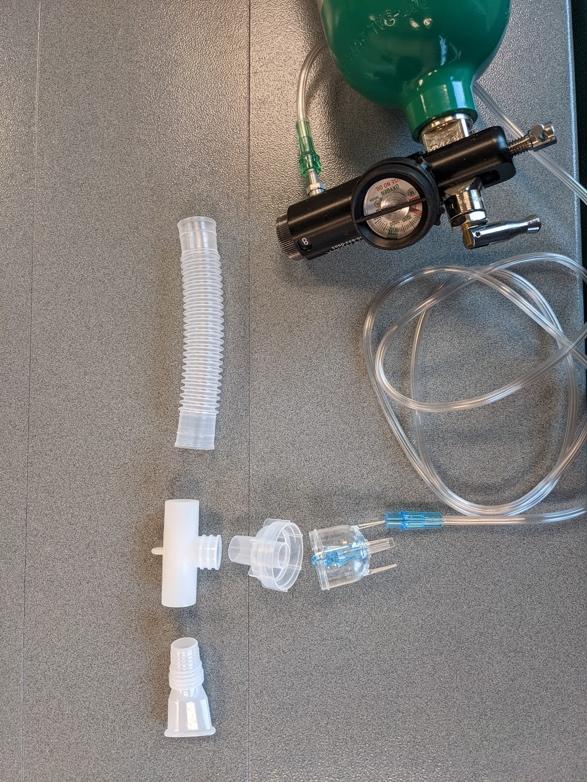
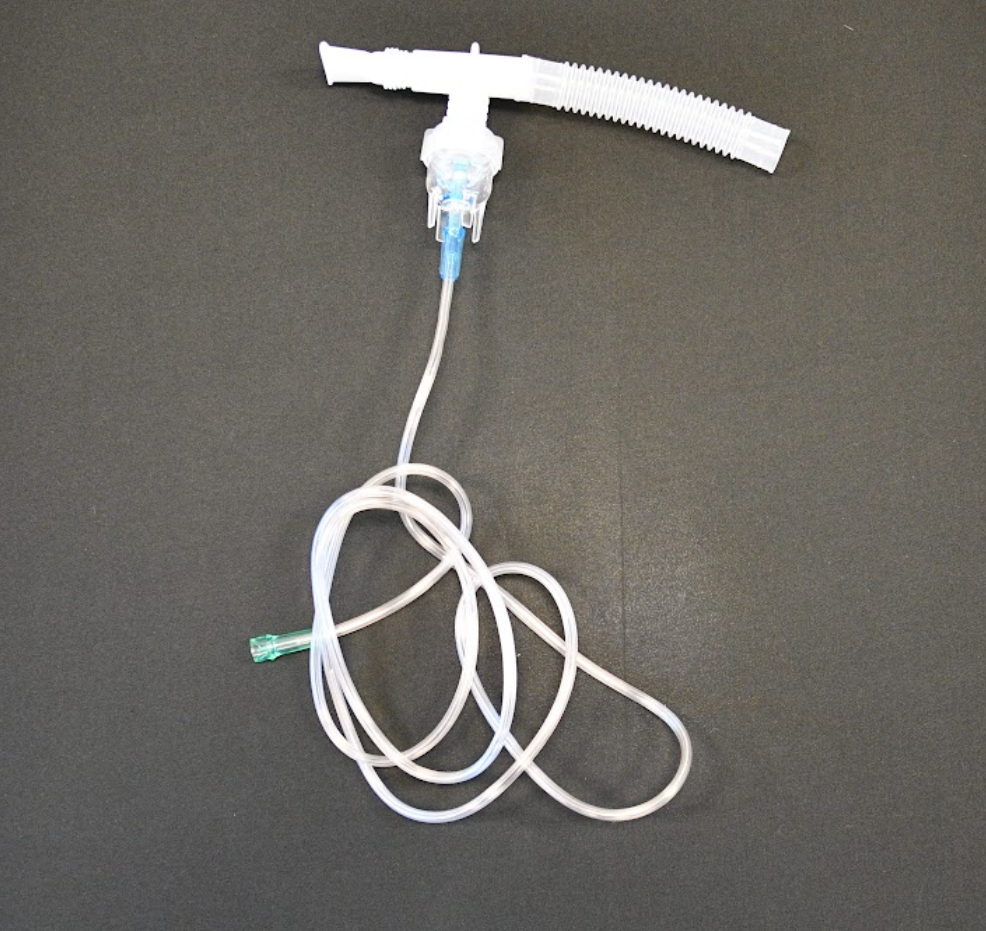
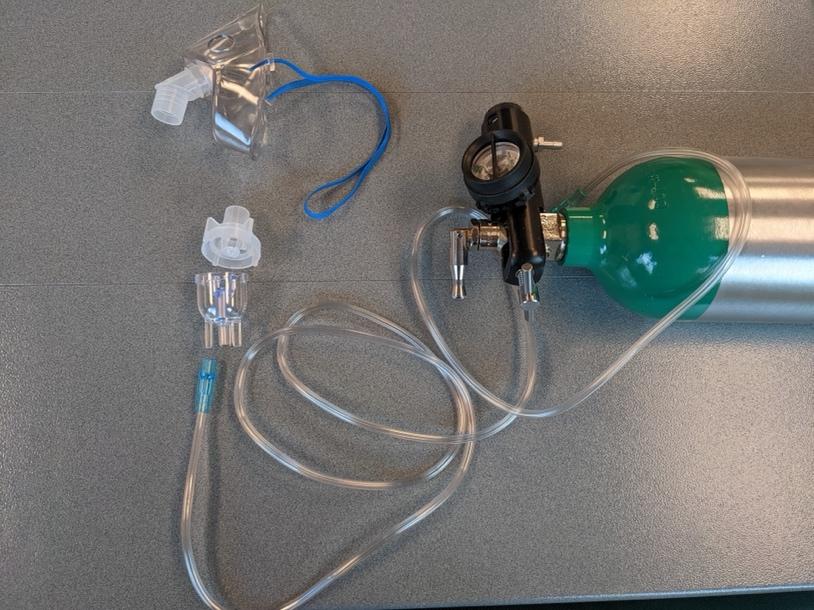
- Assemble equipment (see photo below).
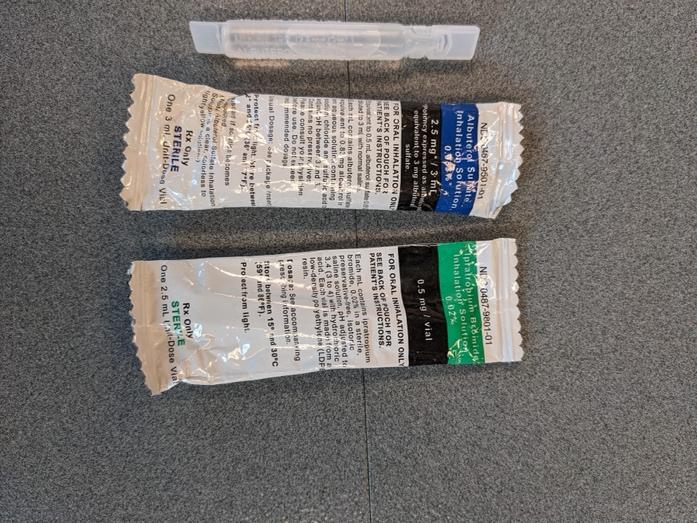
- Insert medication into “acorn” by tearing the top off of a “fish” and squeezing all the contents into container.
- Medication will depend on protocol, though the two common medications are Albuterol and Ipratropium Bromide (see Albuterol & Ipratropium Bromide).
- Screw container together with the rest of the med neb – Note if you skip this step, you will create a mess of medication when you turn on O2.
- Attach oxygen tubing to bottom of “acorn” and set flow rate between 6-8 lpm.
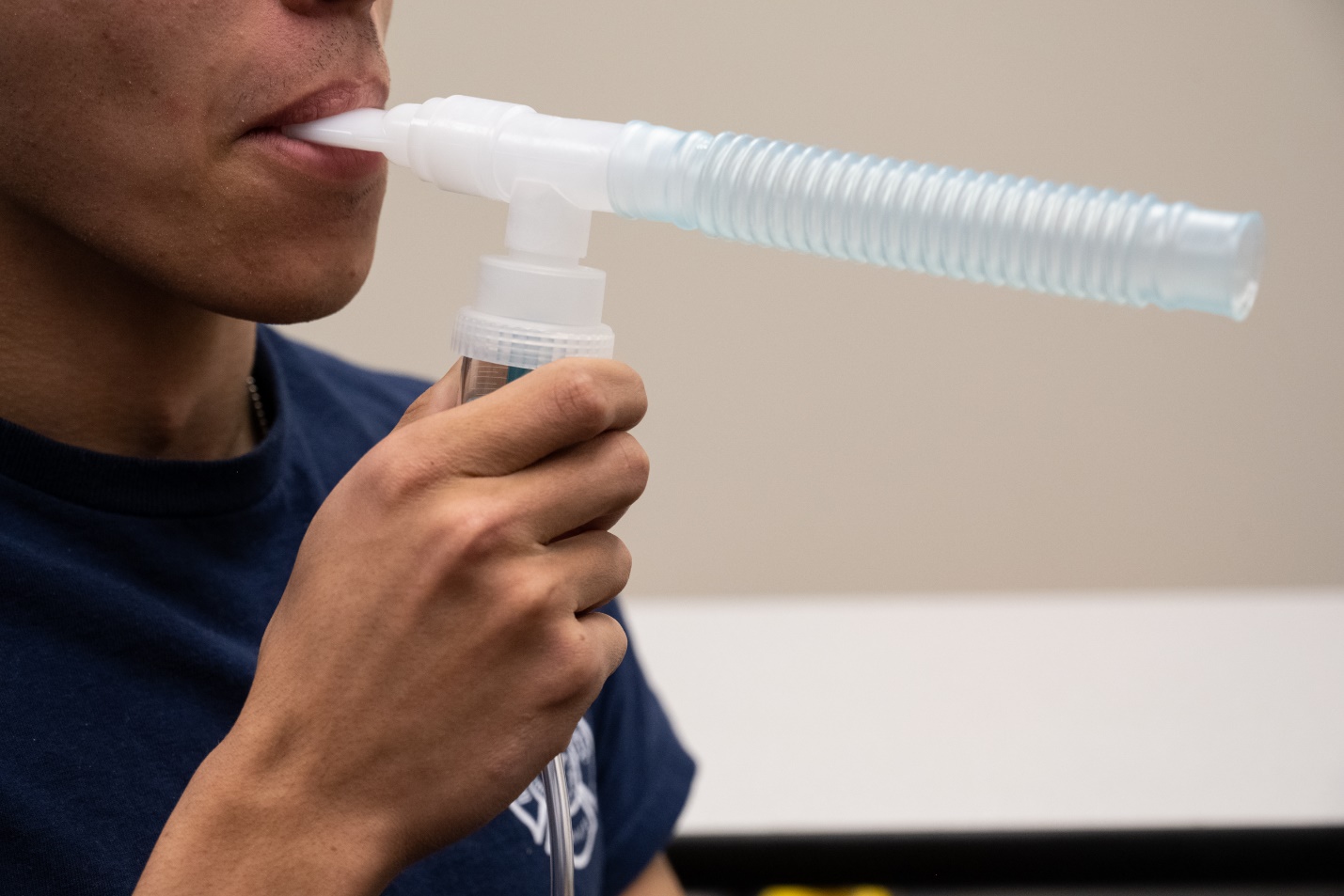
- Instruct patient to hold the med neb in their mouth and take full breaths through the mouthpiece (smaller plastic piece connected to the “T” versus the longer tubing spacer on the other side of the “T”).
- Repeat as necessary, up to your limit by protocol & scope of practice.
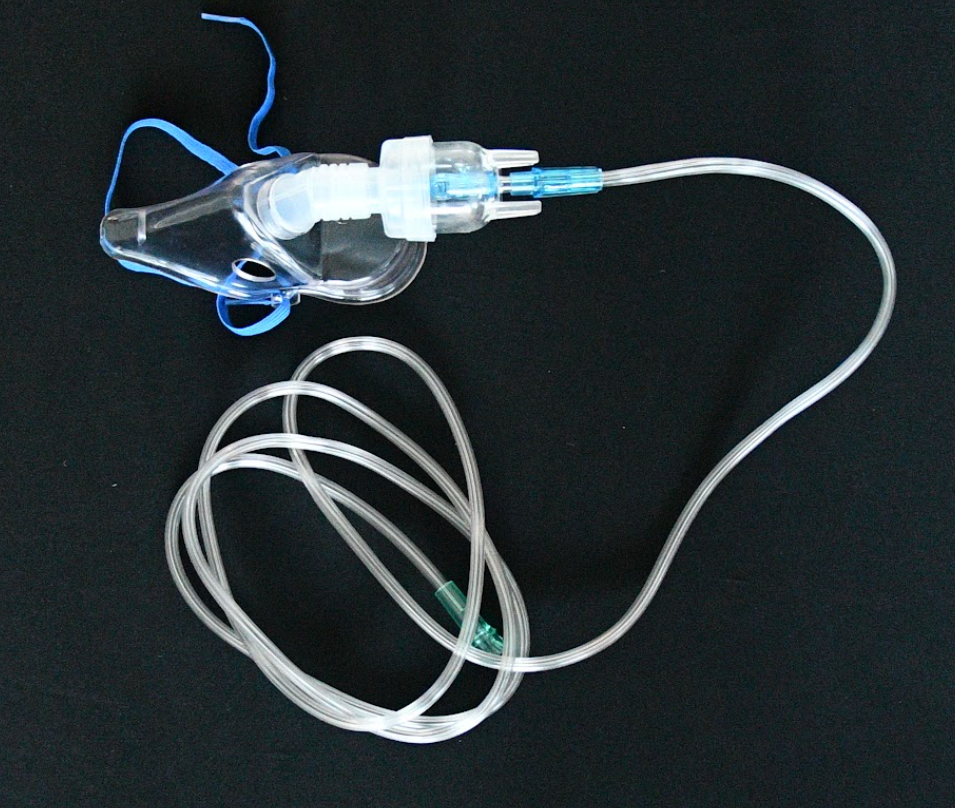
Medication Mask Nebulizer – A medication mask is a variation of the Med-Neb that removes the need for the patient to keep the mouthpiece in their mouth. It delivers the same medications at the same rate as the Med-Neb without the hassle of reminding a forgetful patient and keeps their hands free for other necessary interventions.
Albuterol (Ventolin)
Class: Sympathomimetic (beta-2 agonist)
Mechanism of Action: Bronchodilation by stimulating beta-2 receptors of the bronchi. Has minimal beta-1 (heart) stimulation.
Onset: Immediate
Indications: Known asthma exacerbation, known COPD exacerbation
Contraindications: None in prehospital setting
Side Effects: Hypertension, tachycardia, anxiety, palpitations
Dosage: 2.5 mg in 3 ml saline, supplied in plastic “fish” to be administered in med-neb. Or 1 “puff” of MDI every 3-5 min
|
Albuterol Administration |
1 |
2 |
3 |
4 |
5 (instructor) |
|
Method of Administration |
|
|
|
|
|
|
Initials |
|
|
|
|
|
Ipratropium Bromide (Atrovent)
Class: Anticholinergic bronchodilator, parasympatholytic, antimuscarinic
Mechanism of Action: Ipratropium is a form of atropine given by inhalation. It antagonizes muscarinic cholinergic receptors in the bronchi, producing bronchodilation
Onset: 5-15 minutes
Indications: Known asthma exacerbation, known COPD exacerbation
Contraindications: None
Precautions: Delayed onset of action; not used as sole bronchodilator in emergent setting
Side Effects: Palpitations, anxiety, dizziness
Dosage: 500 mcg nebulized. Usually administered with a β2 agonist (albuterol).
|
Ipratropium Bromide |
1 |
2 |
3 |
4 |
5 (instructor) |
|
Method of Administration |
|
|
|
|
|
|
Initials |
|
|
|
|
|
The original copy of this book resides at openoregon.pressbooks.pub/emslabmanual. If you are reading this work at an alternate web address, it may contain content that has not been vetted by the original authors and physician reviewers.
